Arterial Hypertension in Ukraine: Medical and Social Problems of Pathogenesis
|
Neonila Korylchuk Department of Therapy and Family Medicine, Faculty of Medicine, I.YA. Horbachevsky Ternopil National Medical University of the Ministry of Health of Ukraine, Ternopil, Ukraine.
Roman Riabushko Department of Surgery №1, Poltava State Medical University, Poltava, Ukraine.
Iryna Haman* Department of Propaedeutic of Internal Medicine named after Professor M.M. Berezhnytskyi, Ivano-Frankivsk National Medical University of the Ministry of Health of Ukraine, Ivano-Frankivsk, Ukraine.
Anatolija Krasnova Department of Faculty Therapу, Faculty of Medicine, Uzhhorod National University, Uzhhorod, Ukraine.
Natela Dovzhuk Department of Physiology, Medical Psychological Faculty, Bogomolets National Medical University, Kyiv, Ukraine.
|
*E-mail: [email protected]
Abstract
Arterial hypertension is becoming increasingly common among diseases of the cardiovascular system. The work aimed to analyze blood pressure control in patients diagnosed with arterial hypertension. Fifty physicians and 1020 patients (under 56 years of age) participated in the study. Regular use of medications was observed in 92% of the patients, and the systolic blood pressure level was 167 mm Hg. More frequent use of renin-angiotensin system blockers compared with diuretics and calcium antagonists was noted, both in monotherapy and in combination therapy. Target BP was achieved in 66% of cases within three months by therapy with amlodipine and retarded indapamide. The majority of patients adhered to the prescribed therapy (97%). The effectiveness of amlodipine and indapamide therapy was in direct correlation with baseline BP values. Significant factors were smoking (lower efficacy), and gender (higher in women). The degree of BP reduction following combined therapy with amlodipine and indapamide was determined to be directly correlated with the beginning BP level. At the same time, female patients and non-smokers see more pronounced dynamics of BP lowering. Pre-treatment is also a crucial element; statins and renin system blockers greatly lower blood pressure when used together.
Keywords: Systolic blood pressure level, Diuretics, Monotherapy, Combination therapy, Arterial hypertension
Introduction
Cardiovascular diseases lead to several deaths and disability status all over the world. Ukraine is no exception, where between 1991 and 2013 there was a 2-fold increase in the number of cases of cardiovascular system diseases, up to 5000 thousand for every 100 thousand people (Тatarina, 2022). The distribution of diseases is heterogeneous - while coronary artery disease accounted for 27% of cases, arterial hypertension accounted for 41% of cases during this period (Ghaffar et al., 2021; Maralov, et al., 2022). At the same time, the incidence of ischemia and hypertension in Ukraine has been steadily increasing and has increased by 3.3-3.6 times (Sirenko et al., 2018; Stadniuk et al., 2019). The number of fatal outcomes as of 2012 in Ukraine was 167 for every 100 thousand population (Khomazyuk, & Krotova, 2019). In the EU, the rate is much lower, at 48 cases, and the Eurasian average is 96 cases (Lauder et al., 2020; Yuryk et al., 2022). The level of diabetes mellitus is also high among Ukrainians - this pathology is noted in the 1.4 million population, in Eurasia Ukraine ranks 24th (Mishchenko et al., 2013; Ilina-Stohniienko & Malets, 2022; Kaminskyy & Viesova, 2022). According to the World Health Organization, obesity, diabetes mellitus, and some other pathologies should be considered risk factors for arterial hypertension and coronary artery disease (Nguyen et al., 2021; Tariq et al., 2021). The dynamics of these pathologies are influenced by smoking, being overweight, poor dietary habits, alcoholism, and lack of motivation to exercise (Althobaiti et al., 2021; Shah & Wang, 2022). Due to the fact that the incidence of arterial hypertension in Ukraine remains very high, we can note the lack of effectiveness of measures for primary and secondary prevention of this dangerous disease (Berezin et al., 2021; Gholizadeh et al., 2021).
Theoretical Framework or Literature Review
It is known that each year about 100 thousand Ukrainians suffer strokes. Therefore, the control of blood pressure levels is very important. It is known that the probability of stroke is closely related to systolic blood pressure, as well as to age (Götzinger et al., 2022). If both are high, there is a high probability that cerebral circulation will be impaired. If the elderly observe systolic blood pressure control, the likelihood of stroke is significantly reduced (Hengel et al., 2022). Therefore, therapy recommendations for hypertension need to take the patient's age into account to form the right treatment strategy. Depending on the recommendation, the therapy strategy in relation to age may differ. The age considered as the age limit in the first recommendations was 55 years (Al-Ghorani et al., 2022). These recommendations were developed in the United Kingdom. In the recommendations developed by other European countries, there was no linkage to the age limit, so the therapy strategy was left to the physician. At the same time, it is known that treatment regimens without taking into account the age index can lead not only to the loss of BP control but also to the occurrence of complications (Ott & Schmieder, 2022). In Ukraine, there are still not enough studies devoted to the control of systolic blood pressure levels, especially for the elderly (Khomazyuk, & Krotova, 2019; Tsekhmister et al., 2021). In addition, recommendations for age-appropriate therapy strategies are not always clearly defined, especially in the practice of family physicians and general practitioners. This predetermined the relevance of this study. The study aimed to analyze the level of BP control in an age group of patients aged 55 years and older. The objectives of the study were: a) to study medical and social aspects of pathogenesis; b) to identify possible discrepancies between the existing international recommendations and the proposed treatment regimen; c) to analyze the relationship between the age indicator and the treatment regimen. The obtained results can help to clarify the regional picture of arterial hypertension development, especially taking into account the realities of the war in 2022, which became a stress factor for elderly patients.
Materials and Methods
The study was conducted in 2022 in Ukraine. The study used databases for 50 physicians. The number of general practitioners for each region and the number of patients diagnosed with arterial hypertension are shown in Table 1. The study is retrospective and was conducted in 12 regional centers of Ukraine.
Table 1. Number of doctors and patients who participated in the study
|
Place |
Number of therapists |
Number of patients |
|
1 |
13 |
250 |
|
2 |
7 |
130 |
|
3 |
5 |
110 |
|
4 |
2 |
30 |
|
5 |
5 |
100 |
|
6 |
4 |
90 |
|
7 |
3 |
50 |
|
8 |
2 |
50 |
|
9 |
3 |
50 |
|
10 |
3 |
60 |
|
11 |
2 |
30 |
|
12 |
1 |
20 |
|
Total |
50 |
1020 |
Source: Collected by the authors
Designation: 1 - Kyiv, 2 - Kharkiv, 3 - Dnipro, 4 - Lviv, 5 - Ivano-Frankivsk, 6 - Zhytomyr, 7 - Zaporizhzhia, 8 - Khmelnytskyi, 9 - Mykolaiv, 10 - Chernihiv, 11 - Odesa, 12 - Cherkasy.
All patients who came to see a general practitioner were included in the study. Age (55 years or older) and the diagnosis of arterial hypertension or the presence of blood pressure at 140 over 90 were taken into account. In addition, studies included patients with a history of hypertension who were on antihypertensive therapy. All patients who agreed to participate in the study signed a written contract in which they guaranteed confidentiality and anonymity of the information obtained. The study was conducted following international standards of ethics and morality and was approved at the meeting of the Ethical Committee of the Bogomolets Medical Institute (Kyiv, Ukraine). Of the 1020 patients, 605 were women, and the mean age of all patients was 65 years. The average duration of arterial hypertension disease in the sample was 14 years. We identified such risk factors among the patients as smoking adherence (10%), and the presence of obesity (35%). All patients had high cholesterol levels (average 6.2 mmol per 1 L). Most patients (92%) were on antihypertensive therapy. Twenty percent of patients had a history of diabetes mellitus, 7% had atrial fibrillation, and 13% had a history of stroke. More than half (69%) of the patients had ischemic heart disease, and 21% had a myocardial infarction. The obtained data were processed using Statistics (version 10). We calculated the mean value, standard deviation value, and frequency of birth. We used the Kolmogorov-Smirnov criterion after testing for the normality of the sample distribution. Wilcoxon criterion was used to exclude data with impaired information.
Results and Discussion
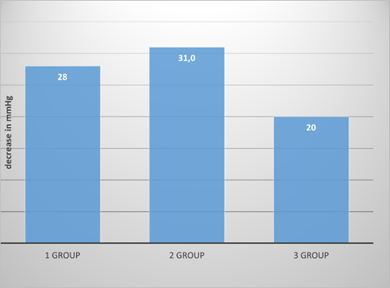
The effectiveness of antihypertensive therapy was found to be inadequate. The difference in mean systolic BP was not significant (168 versus 167 mm Hg in patients who did not take such medications), even though 92% of patients strictly complied with the prescribed therapy regimen. In 7% of cases, patients were able to achieve the suggested BP level while taking antihypertensive medications. According to the results of the Systema study, which included about three thousand patients, those who sought help from a general practitioner had inflated blood pressure readings compared with those who did not (Mishchenko et al., 2013). These patients also rarely had target BP levels (7% vs. 9%). If BP control is at an inadequate level, there may be comorbid cardiovascular abnormalities. These include ischemia (69%), and 21% of patients had complications in the form of a heart attack. 13% of patients had a history of stroke. 8% of patients had atrial fibrillation, which made it difficult to analyze the dynamics of cerebral circulation disorders. We also analyzed the correctness of pretreatment therapy because the wrong strategy can lead to a lack of control of patients' blood pressure levels. International expert recommendations allow for monotherapy if the patient has first-degree arterial hypertension (i.e., arterial systolic pressure levels up to 160 mm Hg) (Paczkowska et al., 2021; Barbosa et al., 2022). In our sample, 19% of patients were correspondingly diagnosed, from which it can be assumed that at least 1 drug lowering the target pressure level was used in their pretreatment. Monotherapy was recorded in 30% of patients, and their systolic blood pressure level corresponded to 165 mmHg. Another 22% of patients used a combination type of therapy, with 39% receiving two drugs and 22% receiving 3 or more. This frequency is roughly in line with that reported in studies from other countries (Castillo & Merlo, 2022; Kockskämper & Pluteanu, 2022). Specifically, in the United States, 28% of patients over 65 years of age took one medication, another 25% took two, and 12% took 3 or more. If BP values are insignificant, lifestyle changes are recommended instead of drug therapy (Hanssen et al., 2022). However, despite the similarity in the frequency of antihypertensive therapy, its effectiveness in the United States is 7 times greater compared to our data in Ukraine - 52%. This may suggest the incorrectness of the chosen drug combinations. For the elderly and old people, it is recommended mainly the use of diuretics and calcium antagonists. Elderly people change their vascular tone, their elastic properties decrease, their stiffness increases, due to which blood pressure increases. There is also a decrease in plasma renin activity, with a parallel decrease in the effect of antihypertensive drugs (Kountouras et al., 2021; Antonazzo et al., 2022). All this served as the basis for the recommendation of diuretics and calcium antagonists because with their help there is a process of vasodilatation of vessels and reduction of BP values. In the presence of diabetes mellitus or other comorbidities, renin-angiotensin system blockers are indicated for elderly and elderly patients diagnosed with arterial hypertension (Sánchez et al., 2020). Prescribing is optimal in the presence of complications such as heart failure (Puszkarska et al., 2019). Our analysis of a sample of patients showed that angiotensin-converting enzyme inhibitors were used in monotherapy (36% of patients) in 28% of cases, and angiotensin 2 blockers were used in only 6% of cases. Diuretics were used only in 1% of cases, whereas calcium antagonists were not prescribed in any patient. It follows that the therapy strategy conformed to international recommendations in only 1% of cases. The condition for compliance was a systolic blood pressure value of 160 mm Hg and there was no need for combination therapy (Ahmed et al., 2023; Al Hamazani et al., 2023; Maneea et al., 2023; Pavithra et al., 2023). When two antihypertensive drugs were used, diuretics and angiotensin-converting enzyme inhibitors (22% of cases) or diuretics and calcium antagonists (6% of cases) were most often used. Angiotensin 2 blockers and diuretics or angiotensin 2 blockers and calcium antagonists were prescribed for 6% of patients (3%). Despite the existing recommendations for elderly patients, no joint treatment with calcium antagonists and diuretics was ever prescribed. In three cases, blockers were prescribed as well as diuretics and calcium antagonists (7% of cases). In the other 8% of cases, no combination of diuretic and calcium antagonist was prescribed. On this basis, we can assume that in the practice of Ukrainian doctors in case of diagnosis of arterial hypertension in a patient aged 55 years and older, only a tenth of them are treated according to the international recommendations with regard to age, i.e., they have prescribed a diuretic and a calcium antagonist. This implies ineffective BP control. Based on our results, we decided to continue the study and held a series of conferences with all participating doctors, in which the recommendations for the therapy of hypertension were discussed in detail, taking into account the age of patients. In the case of a modified therapy approach, diuretics and calcium antagonists were mostly prescribed together (93%); in other cases, other therapy options were chosen. There are drugs such as Arifam, which contains two drugs at once, in this case, amlodipine and indapamide. Most patients (67%) used a ratio of 1.5 to 5.0 mg, another 22% used 1.5 to 10 mg, others chose other ratios. After 90 days, a comparative assessment was made of how effective the therapy had been. The results are shown in Figure 1.
|
|
|
Figure 1. Therapy results of combined use of amlodipine and indapamide in different ratios after 90 days of therapy. 1 - ratio 1.5 to 5.0, 2 - 1.5 to 10.0, 3 - other ratios. |
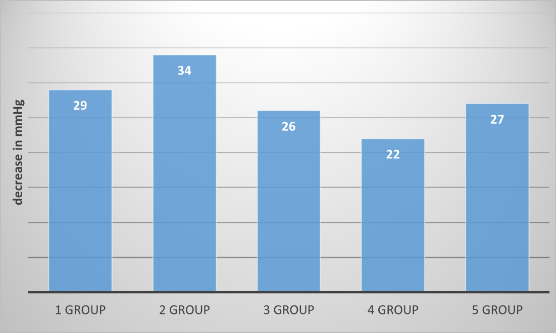
In many cases, the patients managed to achieve the required blood pressure level. A satisfactory level of systolic and diastolic pressure was noted in 68% of patients, 70% of patients with only systolic pressure, and 90% of patients with diastolic pressure. A satisfactory level was understood to be up to 140 by 90 mm Hg. This has been achieved due to the high patient adherence to therapy, the effective action of the combination drug, and the correct age-appropriate therapy. Indapamide promotes the rapid excretion of salts in the urine, which decreases BP and increases diuresis. In addition, the elastic properties of arterial walls are improved, and peripheral vascular resistance is reduced (Huegli & Pechère-Bertschi, 2022). Amlodipine has a relaxing effect on vascular smooth muscle and its use is associated with a reduced risk of stroke (Surma et al., 2021). The high effectiveness of the combined therapy is also evidenced by the fact that after 90 days almost all patients (97%) did not leave the drug. Subsequently, we investigated what factors could reduce the pressure level. It was found that three factors had an influence: a) BP level at the beginning of therapy; b) whether there were other pathologies in the history; c) what therapy preceded the new treatment. In particular, it was found that a higher BP level before the start of therapy was more successful in reducing it during treatment. In the case of baseline systolic blood pressure values within 140-160 mm Hg, the reduction was 19 points, 161-170 - 25 points, 171-180 - 33 points, and from 181 - 44 points. The greatest success was achieved when treatment with renin system blockers was discontinued for the proposed combination. If diuretics and calcium antagonists had previously been used, no such clear reduction was observed (Figure 2).
|
|
|
Figure 2. Blood pressure lowering indexes of amlodipine and indapamide therapy in case of preliminary monotherapy. 1 - angiotensin-converting enzyme inhibitor; 2 - angiotensin 2 blockers; 3 - beta-adrenoblockers; 4 - diuretics; 5 - calcium channel blockers. |
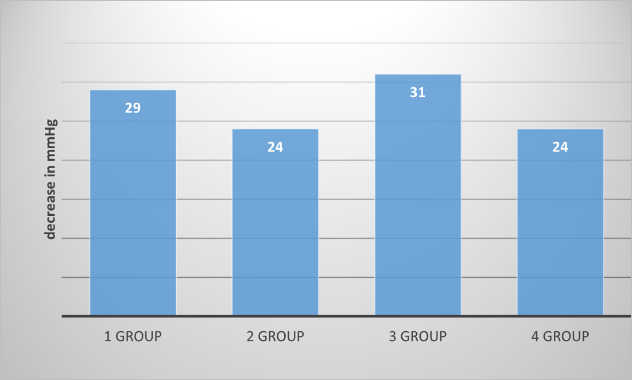
If there was prior therapy with two drugs, a more significant reduction was achieved if a renin system blocker and a diuretic were not present (Figure 3).
|
|
|
Figure 3. Blood pressure reduction indexes of amlodipine and indapamide therapy in case of prior combination therapy. 1 - diuretics and inhibitor; 2 - inhibitor and calcium channel blockers; 3 - angiotensin 2 blockers and diuretics; 4 - angiotensin 2 blockers and calcium channel blockers. |
If patients were on statins, a 3-point reduction in systolic blood pressure was achieved compared with patients whose therapy did not include statins (31 versus 27). The role of statins in enhancing blood pressure-lowering effects is known from the literature (Brosolo et al., 2021; Diaconu et al., 2021; Improta-Caria et al., 2021; Ambatiello et al., 2022). Statins can enhance the antihypertensive effects of other drugs. This may be due to the fact that statins have a positive effect on functional endothelial parameters (Ambatiello et al., 2022). Our study also found a less pronounced effect of amlodipine and indapamide therapy on men, as well as on smokers diagnosed with arterial hypertension. This may be due to the fact that their vascular atherosclerosis is more pronounced.
Conclusion
The level of monitoring of arterial hypertension in Ukraine remains low. On average, according to the literature, the average systolic blood pressure values in patients taking prescribed drugs at the visit of a general practitioner are 168 mm Hg. A decrease in the target values can be achieved only in 7% of cases. In most cases, there is no consideration of the age of patients in accordance with international recommendations. Instead of diuretics, calcium antagonists, or their combination according to international recommendations, Ukrainian therapists most often prescribe renin system blockers. In this regard, it is necessary to reconsider the therapy. In our study, it gave tangible results after 90 days, when the BP level decreased in 67% of patients. 97% of patients were still taking the drug 90 days after the start of therapy. The presence of a direct correlation between the initial BP level and the degree of its reduction after combined therapy with amlodipine and indapamide was established. At the same time, nonsmoking patients and female patients feel more significant dynamics of BP reduction. Pre-treatment is also an important factor - when renin system blockers and statins are present, BP is significantly reduced.
Acknowledgments: The authors are grateful to the anonymous reviewers, whose comments allowed us to improve the quality of the article.
Conflict of interest: None
Financial support: None
Ethics statement: The study was carried out in accordance with international standards of ethics and morality. The study respected the anonymity and confidentiality of the information received.
Ahmed, S., Algarni, T., Alshareef, M., Alhussain, A., Alrashidi, K., & Alahmari, S. (2023). Prevalence of oral mucosal lesions among patients visiting private university dental hospital, Riyadh, Saudi Arabia. Annals of Dental Specialty, 11(1), 83-87. doi:10.51847/qvnfdOmZPj
Al Ghorani, H., Goetzinger, F., Boehm, M., & Mahfoud, F. (2022). Arterial hypertension–Clinical trials update 2021. Nutrition, Metabolism and Cardiovascular Diseases, 32(1), 21-31. doi:10.1016/j.numecd.2021.09.007
Al Hamazani, A., Al Robayaan, A., Al Fuhaid, A., Al Mutairi, F., Mwais, M., Khahtani, N. S. A., Al Amry, H. A., Al Anazi, M. S., & Al Harbi, I. (2023). Dental home care needs among homebound individuals at prince sultan military medical city. Annals of Dental Specialty, 11(1), 78-82. doi:10.51847/1SbFcXeuVl
Althobaiti, A. S. S., Alammari, A. W. A., Ahmed, A. A., Al Saed, S., Saud, M. M., Shaman, S. A. S., & Kamel, O. (2021). Evaluation of the role of antiplatelet medications in cardiovascular disease. Pharmacophore, 12(2), 97-103.
Ambatiello, L. G. (2022). Stress-induced arterial hypertension. Terapevticheskii arkhiv, 94(7), 908-913. doi:10.26442/00403660.2022.07.201733
Antonazzo, B., Marano, G., Romagnoli, E., Ronzoni, S., Frati, G., Sani, G., Janiri, L., & Mazza, M. (2020). Impact of arterial hypertension and its management strategies on cognitive function and dementia: A comprehensive umbrella review. Minerva Cardiology and Angiology, 70(3), 285-297. doi:10.23736/S2724-5683.20.05452-3
Barbosa, S. S., Sousa, L. C. M., de Oliveira Silva, D. F., Pimentel, J. B., Evangelista, K. C. M. D. S., Lyra, C. D. O., Lopes, M. M. G. D. , & Lima, S. C. V. C. (2022). A systematic review on processed/ultra-processed foods and arterial hypertension in adults and older people. Nutrients, 14(6), 1215. doi:10.3390/nu14061215
Berezin, A. А., Myrnyi, D. P., Myrnyi, S. P., & Berezin, A. E. (2021). The hormone-like myokines irisin as novel biomarker for cardiovascular risk stratification. Pharmacophore, 12(1), 44-50.
Brosolo, G., Da Porto, A., Catena, C., & Sechi, L. A. (2021). Arterial stiffening in hypertension: is it just high blood pressure? Reviews in Cardiovascular Medicine, 22(4), 1073-1075. doi:10.31083/j.rcm2204117
Castillo, A. R., & Merlo, A. B. B. (2022). Hipertensión arterial secundaria de etiología infrecuente. Hipertensión y riesgo vascular, 39(2), 92-94. doi:10.1016/j.hipert.2021.09.002
Diaconu, C. C., Cozma, M. A., Dobrică, E. C., Gheorghe, G., Jichitu, A., Ionescu, V. A., Nicolae, A. C., Drăgoi, C. M., & Găman, M. A. (2021). Polypharmacy in the management of arterial hypertension—Friend or foe? Medicina, 57(12), 1288. doi:10.3390/medicina57121288
Ghaffar, F. A., Redzuan, A. M., & Makmor-Bakry, M. (2021). Effectiveness of sildenafil in pulmonary hypertension secondary to valvular heart disease: A systematic review and meta-analysis. Archives of Pharmacy Practice, 12(3), 55-65.
Gholizadeh, B., Nabavi, S. S., Baghaei, S., Zadeh, F. J., Moradi-Joo, E., Amraie, R., Baghaei, A., & Najafian, M. (2021). Evaluation of risk factors for cardiovascular diseases in pregnant women referred to Golestan hospital in Ahvaz. Entomology and Applied Science Letters, 8(3), 40-45.
Goetzinger, F., Kunz, M., Lauder, L., Boehm, M., & Mahfoud, F. (2022). Arterial hypertension-clinical trials update 2022. Hypertension Research, 45(7), 1140-1146. doi:10.1038/s41440-022-00931-2
Hanssen, H., Boardman, H., Deiseroth, A., Moholdt, T., Simonenko, M., Kränkel, N., Niebauer, J., Tiberi, M., Abreu, A., Solberg, E. E., et al. (2022). Personalized exercise prescription in the prevention and treatment of arterial hypertension: A consensus document from the european association of preventive cardiology (EAPC) and the ESC council on hypertension. European Journal of Preventive Cardiology, 29(1), 205-215. doi:10.1093/eurjpc/zwaa141
Hengel, F. E., Sommer, C., & Wenzel, U. (2022). Arterial hypertension. Deutsche Medizinische Wochenschrift (1946), 147(7), 414-428. doi:10.1055/a-1577-8663
Huegli, S., & Pechère-Bertschi, A. (2022). L’hypertension artérielle a-t-elle un genre? Revue Medicale Suisse, 18(795), 1689-1692. doi:10.53738/revmed.2022.18.795.1689
Ilina-Stohniienko, V., & Malets, M. (2022). Regarding the modernization of the medical care system for victims of armed conflicts (Ukrainian experience). Futurity Medicine, 1(3), 30-42. doi:10.57125/FEM.2022.09.30.04
Improta-Caria, A. C., Aras, M. G., Nascimento, L., De Sousa, R. A. L., Aras-Júnior, R., & Souza, B. S. D. F. (2021). MicroRNAs regulating renin–angiotensin–aldosterone system, sympathetic nervous system and left ventricular hypertrophy in systemic arterial hypertension. Biomolecules, 11(12), 1771. doi:10.3390/biom11121771
Kaminskyy, V., & Viesova, O. (2022). Innovative activities in healthcare institutions of the future: Models for overcoming dilemmas. Futurity Medicine, 1(1), 17-26. doi:10.57125/FEM.2022.03.25.02
Khomazyuk, T. А., & Krotova, V. Y. (2019). Quality of life and cognitive health in hypertension: is it possible? Medicine of Ukraine, 0(3(229)), 16-18. doi:10.37987/1997-9894.2019.3(229).185087
Kockskämper, J., & Pluteanu, F. (2022). Left atrial myocardium in arterial hypertension. Cells (Basel, Switzerland), 11(19), 3157. doi:10.3390/cells11193157
Kountouras, J., Papaefthymiou, A., Polyzos, S. A., Deretzi, G., Vardaka, E., Soteriades, E. S., Tzitiridou-Chatzopoulou, M., Gkolfakis, P., Karafyllidou, K., & Doulberis, M. (2021). Impact of Helicobacter pylori-related metabolic syndrome parameters on arterial hypertension. Microorganisms, 9(11), 2351. doi:10.3390/microorganisms9112351
Lauder, L., Azizi, M., Kirtane, A. J., Boehm, M., & Mahfoud, F. (2020). Device-based therapies for arterial hypertension. Nature Reviews Cardiology, 17(10), 614-628. doi:10.1038/s41569-020-0364-1
Maneea, A. S. B., Alqahtani, A. D., Alhazzaa, A. K., Albalawi, A. O., Alotaibi, A. K., & Alanazi, T. F. (2023). Microbiological Effect of Various Concentrations of Sodium Hypochlorite (NaOCL) During Endodontic Treatment: A Systematic Review. Annals of Dental Specialty, 11(1), 95-101. doi:10.51847/7CZTguksH9
Maralov, V. G., Sitarov, V. A., Koryagina, I. I., Kudaka, M. A., Smirnova, O. V., & Romanyuk, L. V. (2022). The relationship of neuropsychological and personal factors with the attitude to dangers among students. Journal of Organizational Behavior Research, 7(1), 108-124.
Mishchenko, O. Ya, Іakovlіeva, L. V., Adonkina, V. Yu., & Chinush, I. V. (2013). Pharmacoepidemiological research of the use of antihypertensive drugs in Ukraine. Pharmaceutical Journal (Uzbekistan), 1, 4-9. https://dspace.nuph.edu.ua/handle/123456789/3455
Nguyen, S. N., Le, T. T. M., Nga, H. T., & Tho, N. T. T. (2021). Lifestyle interventions reduce the risk of type II diabetes and cardiovascular diseases development among pre-diabetic adults. International Journal of Pharmaceutical Research & Allied Sciences, 10(2), 94-102.
Ott, C., & Schmieder, R. E. (2022). Diagnosis and treatment of arterial hypertension 2021. Kidney International, 101(1), 36-46. doi:10.1016/j.kint.2021.09.026
Paczkowska, A., Hoffmann, K., Kus, K., Kopciuch, D., Zaprutko, T., Ratajczak, P., Michalak, M., Nowakowska, E., & Bryl, W. (2021). Impact of patient knowledge on hypertension treatment adherence and efficacy: A single-centre study in Poland. International Journal of Medical Sciences, 18(3), 852-860. doi:10.7150/ijms.48139
Pavithra, A. S., Paulraj, J., Rajeshkumar, S., & Maiti, S. (2023). Comparative evaluation of antimicrobial activity and compressive strength of conventional and thyme-modified glass ionomer cement. Annals of Dental Specialty, 11(1), 70-77. doi:10.51847/FrmCSw6TqP
Puszkarska, A., Niklas, A., Głuszek, J., Lipski, D., & Niklas, K. (2019). The concentration of tumor necrosis factor in the blood serum and in the urine and selected early organ damages in patients with primary systemic arterial hypertension. Medicine, 98(22), e15773. doi:10.1097/MD.0000000000015773
Sanchez, R. A., Boggia, J., Penaherrera, E., Barroso, W. S., Barbosa, E., Villar, R., Cobos, L., Hernandez Hernandez, R., Lopez, J., Octavio, J. A., et al. (2020). Ambulatory blood pressure monitoring over 24 h: A Latin American society of hypertension position paper—Accessibility, clinical use and cost effectiveness of ABPM in Latin America in year 2020. The Journal of Clinical Hypertension, 22(4), 527-543. doi:10.1111/jch.13816
Shah, R. T., & Wang, B. X. (2022). Effectiveness of renal denervation in the treatment of hypertension: A literature review. Clinical Hypertension, 28(1), 11. doi:10.1186/s40885-022-00194-6
Sirenko Yu. M., Mishchenko L. A., Radchenko H. D., Kupchynska O. H., Rekovets O. L., & Kushnir S. M. (2018). Classification and standards of medical care for patients with arterial hypertension of the Association of Cardiologists of Ukraine. Arterial Hypertension, (4 (60)), 26-47.
Stadniuk, L. A., Kononenko, O. A., Oliinyk, M. V., Davydovych, O. V., & Mikropulo, I. R. (2019). Cardiovascular risk and condition of target organs in patients of various ages with hypertension and high normal or low normal levels of TSH. Family Medicine, 0(1), 71-75. doi:10.30841/2307-5112.1.2019.172210
Surma, S., Romańczyk, M., Witalińska-Łabuzek, J., Czerniuk, M. R., Łabuzek, K., & Filipiak, K. J. (2021). Periodontitis, blood pressure, and the risk and control of arterial hypertension: Epidemiological, clinical, and pathophysiological aspects—review of the literature and clinical trials. Current Hypertension Reports, 23(5), 27. doi:10.1007/s11906-021-01140-x
Tariq, A., Fuad, A., Hanan, A., Waleed, A., & ElShaer, F. (2021). Estimation of left ventricular filling pressure by assessment of left atrial contractile function using cardiovascular magnetic resonance volumetry. International Journal of Pharmaceutical Research and Allied Sciences, 10(1), 1-6.
Tatarina O. (2022). Innovations in Ukrainian medicine: Priorities, directions, and forecasts. Futurity Medicine, 1(3), 42-51. doi:10.57125/FEM.2022.09.30.05
Tsekhmister, Y., Stepanenko, V., Konovalova, T., & Tsekhmister, B. (2021). Pharmaco economics analysis of COVID-19 vaccines in Ukraine. Journal of Pharmaceutical Research International, 33(32A), 140-147. doi:10.9734/jpri/2021/v33i32A31727
Yuryk, O., Barabanchyk, O., & Malets, M. (2022). Innovations in medicine: Modern challenges, future definitions: A narrative review. Futurity Medicine, 1(2), 23-30. doi:10.57125/FEM.2022.06.30.03