Antimicrobial Potential of Azadirachta indica (Neem) Leaves Extracts Against Various Pathogenic Bacteria
Asmaa Wasl Almaghamsi, Munazza Gull*, Ebtihaj Jambi, Ahmed Al-Hejin, Noor M. Bataweel, Shaza Yehya Abdulhamed Qattan
Abstract
Antimicrobial resistance has become a serious threat to human health nowadays. This research aimed to explore the potential of plants to be used as antimicrobial agents against pathogenic bacteria. Three different extracts of Azadirachta indica (Neem) leaves (methanolic, ethanolic, and aqueous) were tested against 5 Gram-positive and 4 Gram-negative bacteria. For Gram-positive bacteria, ethanolic extract showed the best antimicrobial potential. Bacillus cereus was found more sensitive to ethanolic extract at 500 mg/ml conc. with a 21.1 mm zone of inhibition. For methanolic extract, at 500 mg/ml conc. Bacillus cereus and Methicillin-resistant Staphylococcus aureus were found more sensitive with 15.4 mm and 15.1 mm ZOI, respectively. Streptococcus pneumoniae was resistant to methanolic Neem extract. Three Gram negative bacteria: Klebsiella pneumoniae, Escherichia coli, and Salmonella typhimurium were resistant to all Neem leaves extracts. The best antimicrobial results of ethanolic and methanolic extracts against Pseudomonas aeruginosa were at 200 mg/ml conc. of each extract with 18.3 and 21.2 mm ZOI, respectively. Negative results were found for aqueous extract with all tested pathogenic bacteria. HPLC analysis of Neem leaves extracts depicted that benzoic acid was detected in ethanolic extract, while ferulic acid and 4-hydroxy benzoic acid were found in all three Neem leaf extracts. This study confirmed the antibacterial activity of Neem leaves against these bacterial strains and the possibility of employing this knowledge in new antibacterial drug development.
Keywords: Antimicrobial, Azadirachta indica, HPLC, Medicinal plants, Neem
Introduction
Globally, antimicrobial resistance (AMR) threatens the health of populations, especially in developing countries, making it difficult to treat and control many infectious diseases (Iwu-Jaja et al., 2021).
Although the rise and spread of antimicrobial resistance occur naturally, the problem is exacerbated by the misuse and overuse of antibiotics in humans and animals (Ren-Zhang et al., 2020). By 2050, Approximately 10 million people might reach to death from AMR and the economic cost will reach US$100 trillion (Matos de Opitz & Sass, 2020). According to WHO (World Health Organization) report, there are alarming levels of antibiotic resistance in several parts of the world, with up to 54% of resistance to third-generation cephalosporins and carbapenems (World Health Organization, 2014). The high incidence of antimicrobial resistance negatively affects the quality of treatment, causing complications and severe outcomes (Adlan et al., 2021; Assaggaf, 2021). The result is an increase in hospitalizations and unnecessary costs for health facilities and patients, eventually, resulting in the end of the antibiotic era. People who are not directly exposed to antimicrobials can also be harmed by improper use (Al-Ghamdi et al., 2020; Tiwari et al., 2020). Therefore, utilizing these drugs effectively will enhance patient safety, ensure that antibiotics are sustainable for as long as possible, and reduce catastrophic healthcare costs (Andersson & Hughes, 2011).
In 2017, the WHO published a list of bacteria that are considered priority pathogens due to their antibiotic resistance. It consists of 12 different families of bacteria that are considered to be the highest health risks and pose a particular threat in hospitals, nursing homes, and patients with blood catheters or ventilators. These bacteria including Pseudomonas, Acinetobacter, and various Enterobacteriaceae (e.g., E. coli, Serratia, Klebsiella, and Proteus) have developed resistance to a wide variety of antibiotics, including carbapenems and third-generation cephalosporins. Pneumonia and bloodstream infections are among the serious and often fatal infections they can cause (Tacconelli et al., 2018).
Since primitive times, humans have been searching in nature for resources that permit them to improve living conditions and consequently, prolong their life span. Some of the plants emerging today as potential therapeutic agents were already recognized in the past; however, the reason behind their therapeutic use was not fully understood at that time (Fernandes et al., 2019).
The medicinal plant is a term used to describe a type of plant with pharmacological activity to treat diseases. Azadirachta indica (A. indica) is a large evergreen Indian tree from the Meliaceae family, commonly known as “Neem”. It has a wide spectrum of biological activities which make it well-known in India as a medicinal plant over the years. It is also used in agriculture because of its pesticide activity against more than 400 insect pests and in cosmetics. The height of the Neem tree is about 20 m and it can live and provide shade for more than 150 years (Alves et al., 2009).
Each part of the tree has its biological properties and benefits. Azadirachta indica parts include leaves, flowers, seeds, fruits, roots, and bark. A. indica leaf has the most medicinal utility. Its constituents include carbohydrates, crude proteins, crude fibers, fats, and minerals. It also contains phytochemicals such as desactylimbin, sitosterol, terpenoids, and quercetin. Studies have shown immunomodulatory, anti-inflammatory, antioxidant, antifungal, antibacterial, neuropharmacological, antihyperglycaemic, antiulcer, antimalarial, antiviral, antimutagenic, and anticarcinogenic properties for A. indica leaves (Gupta et al., 2017).
Azadirachtin (AZA) is the main active compound in the Azadirachta indica plant, it is usually used as a biological marker for this plant. It presents mostly in seeds and low levels in leaves. Other active compounds in Azadirachta indica extracts include gedunin, Nimbin, azadiractol, melianone, meliantrol, azadirone, vilosinin, and many others. Azadirachta indica extracts are a natural alternative to conventional pesticides which affect the ecosystem and the environment negatively (Fernandes et al., 2019).
The world health organization (WHO) estimates that 80% of the population living in developing countries relies exclusively on traditional medicine for their primary health care. More than half of the world’s population still relies entirely on plants for medicines, and plants supply the active ingredients of most traditional medical products. Researchers generally agree that natural products from plants and other organisms have been the most consistently successful source for ideas for new drugs. Drug discovery scientists often refer to these ideas as “leads,” and chemicals that have desirable properties in lab tests are called lead compounds (Kumar & Navaratnam, 2013).
In recent years, the number of people killed by infectious diseases has been raised due to drug-resistant bacteria and fungal pathogens. Producing new antimicrobial drugs is necessary (Khursheed & Jain, 2021). The medicinal plant is a good choice because of the therapeutic properties of its components. Useful components can inhibit the growth of pathogens or kill them with no or least toxicity to the host cells (Uzzaman, 2020).
Materials and Methods
Azadirachta Indica Extracts Preparation
Azadirachta indica (Neem) leaves were collected from Jeddah city, Saudi Arabia. A. indica leaves were divided into 3 groups (500 g of each). They washed to remove dust, dried in the shade, and ground into powder. The powder of each group was added to 1 L of ethanol (99.8%), methanol (≥99.8%), and distilled water, respectively. After 3-day shaking using a normal shaker, the products were filtered to get the extracts. CentriVap Concentrator and Lyophilizer were used to remove the solvents. Three different concentrations of each extract were tested against pathogenic bacteria: 100, 200, and 500 mg dissolved in 1 mL of the same solvent.
High-Performance Liquid Chromatography (HPLC)
HPLC study was performed to identify the presence of phenolic compounds in A. indica extracts.
Preparation of Sample and Standard Solutions
For sample stock preparation, an amount of 50 mg of each A. indica extract were dissolved in 100 mL of extraction solvent using vortex mixing and a shaker. A concentration of 400μg/mL was obtained by diluting 40mL of each stock solution in 50mL of the same solvent. The standard stock solutions of gallic acid, ferulic acid, chlorogenic acid (LKT Laboratories, INC., USA), benzoic acid (Techno Pharmchem, India), and parahydroxy benzoic acid (Acros Organics, Belgium) were prepared by dissolving 50 mg of each standard in 100 mL of methanol (HPLC grade). A concentration of 50 μg/mL was obtained by diluting 5 mL of each stock solution in 50 mL of methanol. All 8 samples and standard solutions were passed through a 0.45 μm disposable membrane filter before HPLC analyses.
Analyses by HPLC
A. Indica leaves extracts were tested by reverse phase-high performance liquid chromatography (HPLC). The analyses were performed on Shimadzu HPLC equipped with a quaternary pump, automatic injector, and a photodiode array detector (PDA) module. (El-Sokkary, 2023). Separations were achieved using a C18 column (Agilent, 4.6 × 150 mm) subjected to gradient elution. LC solution software was used for data acquisition. Mobile phase: Water +1% Trifluoroacetic Acid (Line A) and Acetonitrile (Line B) at 1.0 mL/min flow rate, and 5 µL injection volume were used. The samples were analyzed using a PDA detector in scan mode covering the range of 200-400 nm.
Antimicrobial Potential Evaluation
Bacterial Strains and Media
Nine clinically isolated and identified pathogenic bacterial strains (5 Gram-positive and 4 Gram-negative bacteria) were obtained from the Microbiology laboratory at King Fahad Medical Research Center (KFMRC), Jeddah, Saudi Arabia. Media used to grow bacteria were purchased from TM Media, India, and prepared according to the manufacturer’s instructions. Nutrient agar was used to grow the following pathogenic bacteria: Escherichia coli (ATCC 25922), Staphylococcus aureus (ATCC 29213), Klebsiella pneumoniae (ATCC 5205773), Bacillus subtilis, Bacillus cereus (ATCC 115714), Salmonella enterica ser. typhimurium (ATCC 14028), Pseudomonas aeruginosa (ATCC 9027), MRSA (ATCC 33591), and Streptococcus pneumoniae (ATCC 49619). The cultures were maintained at 4°C on nutrient agar slants. Stock bacterial cultures were preserved in 50% glycerol at -20°C for long-term storage.
In vitro Antibacterial Activity Evaluation
The agar well diffusion method was used as described by Nalawade et al. (2016) to evaluate the antibacterial activity of A. indica leaves extracts. The best medium to use for in vitro susceptibility testing is Muller-Hinton Agar (MHA). Ciprofloxacin (5μg/mL) and Kanamycin (30μg/mL) discs were purchased from Bioanalyse, Turkey, and used as a standard positive control.
For suspension preparation, bacterial colonies were transferred using inoculating loops from Nutrient agar plates to sterile saline. Then, a sterile cotton swab (Citotest) was dipped in the suspension and used to spread the bacteria evenly on the entire surface of the MHA plate. A sterile cork borer (7mm) (Thomas Scientific) was used to make 3 wells in each plate. Each well was filled with 100 µl of the extract and incubated overnight at 36±1.00C. The diameter of each inhibition zone was measured in mm using a ruler and recorded in the recording sheet. Three different concentrations (100, 200, and 500 mg/ml) of each extract (ethanolic, methanolic, and aqueous Neem extracts) were tested against 9 pathogenic bacteria, in triplicate. The results were expressed as the average diameter of inhibition zones in mm ± standard error of the mean (SEM) and compared to the standard antibiotics (positive control), Ciprofloxacin (5μg/mL), and Kanamycin (30μg/mL). As a negative control, solvents used in extract preparation (ethanol (99.8%), methanol (≥99.8%), and distilled water) were tested against all pathogenic bacteria.
Statistical Analysis
The statistical analysis was performed using Windows Microsoft 365 Excel software. The results were expressed as mean ± standard deviation (SD). The data were subjected to One-Way Analysis of Variance (ANOVA) to determine the individual difference at p ˂ 0.05 level.
Results and Discussion
Analyses by HPLC
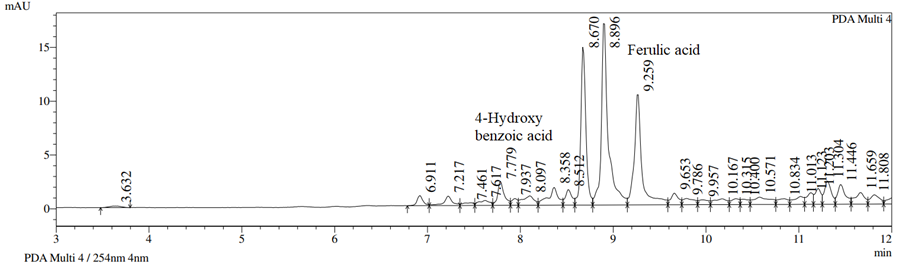
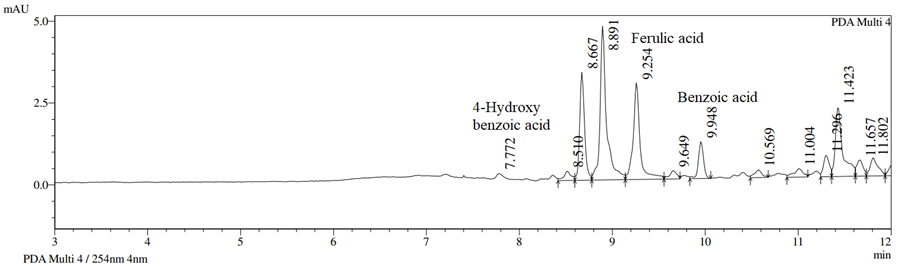
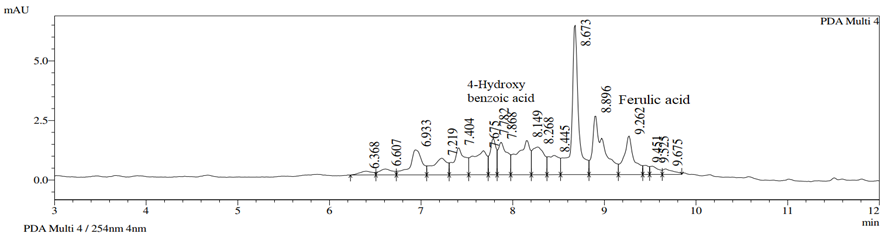
Analysis of A. indica leaves extracts was carried out based on chromatographic separation. Five phenolic compounds including gallic acid, benzoic acid, ferulic acid, chlorogenic acid, and 4-hydroxybenzoic acid were analyzed under identical conditions. The presence of gallic acid and chlorogenic acid was not reported for any of the A. indica leaves extracts. Ferulic acid and 4-hydroxy benzoic acid were detected in all three A. indica leaves extracts with retention time tR= 9.25 min, and tR= 7.77 min, respectively (Figures 1-3). Qualitative analysis of A. indica leaves extracts depicted that benzoic acid was detected in an ethanolic extract with retention time tR= 9.96 min (Figure 2). These results indicated that the presence of these phenolic compounds in A. indica leaves extracts made it a strong antimicrobial agent and these phenolic compounds could be a great source in future drug development projects.
Antimicrobial Potential of Azadirachta indica Leaves Extracts
Three different extracts of Azadirachta indica leaves were tested against the following nine pathogenic bacteria; Escherichia coli (ATCC 25922), Staphylococcus aureus (ATCC 29213), Klebsiella pneumoniae (ATCC 5205773), Bacillus subtilis, Bacillus cereus (ATCC 115714), Salmonella enterica ser. typhimurium (ATCC 14028), Pseudomonas aeruginosa (ATCC 9027), MRSA (ATCC 33591), and Streptococcus pneumoniae (ATCC 49619).
|
|
|
Figure 1. HPLC chromatogram of methanolic A. indica extract (400 μg/mL) recorded at 254 nm indicating the presence of 4-hydroxy benzoic acid and ferulic acid. |
|
|
|
Figure 2. HPLC chromatogram of ethanolic A. indica extract (400 μg/mL) recorded at 254 nm indicating the presence of 4-hydroxy benzoic acid, ferulic acid, and benzoic acid. |
|
|
|
Figure 3. HPLC chromatogram of aqueous A. indica extract (400 μg/mL) recorded at 254 nm indicating the presence of 4-hydroxy benzoic acid and ferulic acid. |
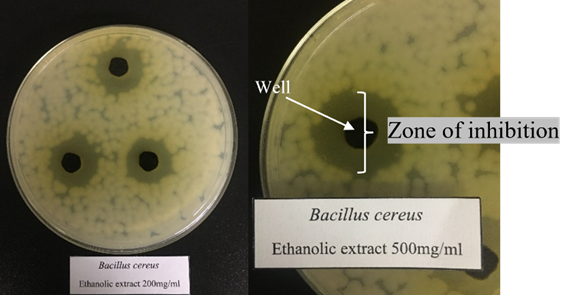
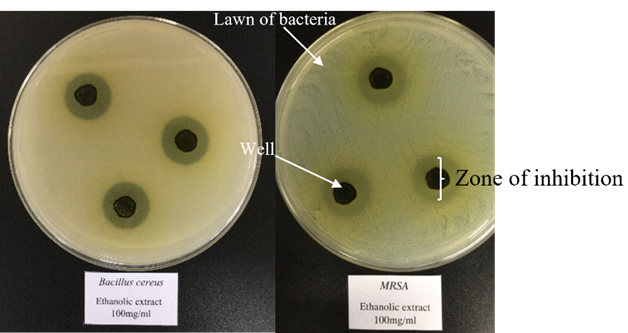
It has been observed that ethanolic extract showed the best antimicrobial potential compared to other extracts. At 100 mg/ml conc. Bacillus cereus and MRSA were found more sensitive to ethanolic Neem extract with 16.1 and 16 mm zone of inhibition (ZOI), respectively (Figure 4). Bacillus cereus was also the most sensitive bacteria to 200 mg/ml conc. and 500 mg/ml conc. ethanolic extract with 18.7 and 21.1mm zone of inhibition, respectively (Figure 5). For methanolic extract, at 100 mg/ml conc. MRSA was found more sensitive with a 14.2 mm zone of inhibition. At 200 mg/ml conc. and 500 mg/ml conc. Bacillus cereus and MRSA were found more susceptible. The zone of inhibition for Bacillus cereus was found 14.9 mm at 200 mg/ml conc. and 15.4 mm at 500mg/ml concentration. For MRSA, the zone of inhibition was observed at 14.7 mm at 200mg/ml conc. and 15.1mm at 500 mg/ml conc. Streptococcus pneumoniae was resistant to methanolic Neem extracts with no zone of inhibition with all concentrations (Table 1).
Three Gram-negative bacteria; Klebsiella pneumoniae, Escherichia coli, and Salmonella enterica ser. Typhimurium was resistant to all A. indica leaves extracts. Both ethanolic and methanolic extracts showed antimicrobial effects on Pseudomonas aeruginosa with more sensitivity for methanolic extract. The best antimicrobial results of Neem ethanolic and methanolic extracts against Pseudomonas aeruginosa were at 200 mg/ml conc. of each extract with 18.3 and 21.2 mm zone of inhibition, respectively. Negative results with no zone of inhibition were found for aqueous extract with all tested pathogenic bacteria (Table 1). Post hoc analysis of One-Way ANOVA between bacterial strains indicated that there is a statistically significant difference at alpha = 0.05, p= 4.10-6 between tested pathogenic bacteria (Feghhi et al., 2022; Nurcahyo et al., 2022; Rahayuningtyas et al., 2022; Deisy et al., 2023; Gofur et al., 2023; Tawfik et al., 2023). As a negative control, solvents used in extract preparation were tested against all pathogenic bacteria and showed no effect on bacterial growth with no zone of inhibition. Two antibiotics: kanamycin (30μg/mL), and ciprofloxacin (5μg/mL) were tested against all pathogenic bacteria as a positive control. The best results were observed for ciprofloxacin against Bacillus subtilis and Escherichia coli with 33 and 31mm zone of inhibition, respectively. Bacillus subtilis and Escherichia coli were also sensitive to kanamycin with 23 and 20 mm zone of inhibition, respectively. Streptococcus pneumoniae, Salmonella enterica ser. Typhimurium and Pseudomonas aeruginosa were resistant to kanamycin with no zone of inhibition. Diameters of inhibition zones of blanks and standard antibiotics have been shown in Table 2.
HPLC is a sensitive and accurate tool that is widely used for the quality assessment of plant extract and its derived product/formulation. Reversed phase-HPLC with C18 columns is the most popular technique for the analysis of polyphenols of different food (Supritha & Radha, 2018). Various solvents of different polarities must be used to extract various phenolic compounds from plants with a high degree of accuracy. Solvents used for the extraction of biomolecules from plants are chosen based on the polarity of the solute of interest. A solvent of similar polarity to the solute will properly dissolve the solute. The polarity, from least polar to most polar, of a few common solvents is as follows: Hexane < Chloroform < Ethyl acetate < Acetone < Methanol < Water (Mohankumar et al., 2020).
Table 1. Antimicrobial activity of Azadirachta indica leaves extracts
|
A. indica extract |
Concentration |
Inhibition zone (mm) |
||||||||
|
Gram-Positive bacteria |
Gram-Negative bacteria |
|||||||||
|
B. cereus |
B. subtilts |
S. pneumoniae |
S. aureus |
MRSA |
S. Typhi |
K. pneumonia |
E. coli |
P. aeruginosa |
||
|
Ethanol |
100 |
16.1± 0.3 |
12.4± 0.5 |
11.6± 0.5 |
15.0± 0.5 |
16.0± 0.5 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
16.2± 2.9 |
|
200 |
18.7± 0.7 |
14.0± 0.0 |
11.3± 0.5 |
15.3± 0.5 |
16.4± 1.1 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
18.3± 2.7 |
|
|
500 |
21.1± 1.2 |
14.7± 0.5 |
11.3± 0.5 |
14.8± 0.4 |
16.4± 0.5 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
16.4± 0.7 |
|
|
Methanol |
100 |
13.0± 0.7 |
10.9± 0.3 |
0.0± 0.0 |
13.1± 1.1 |
14.2± 0.7 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
18.3± 2.0 |
|
200 |
14.9± 0.9 |
12.9± 0.6 |
0.0± 0.0 |
14.3± 2.0 |
14.7± 0.5 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
21.2± 1.8 |
|
|
500 |
15.4± 0.5 |
14.7± 0.5 |
0.0± 0.0 |
13.0± 0.0 |
15.1± 2.5 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
20.0± 2.1 |
|
|
Aqueous |
100 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
|
200 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
|
|
500 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
0.0± 0.0 |
|
The table shows the mean value of inhibition zone diameter in mm. Data are means of three replicates (n=3) ± standard error.
0.0 = No inhibition zone (Resistant).
Table 2. The inhibition zones diameter of blanks and standard control antibiotics against different pathogenic bacteria (mm)
|
Bacteria |
Standard antibiotics (Positive control) |
Blank (Negative control) |
|||
|
Kanamycin (30 μg/mL) |
Ciprofloxacin (5 μg/mL) |
Ethanol |
Methanol |
Distilled water |
|
|
Bacillus cereus |
15 |
28 |
0.00 |
0.00 |
0.00 |
|
Bacillus subtilis |
23 |
33 |
0.00 |
0.00 |
0.00 |
|
Streptococcus pneumoniae |
0 |
21 |
0.00 |
0.00 |
0.00 |
|
Staphylococcus aureus |
18 |
26 |
0.00 |
0.00 |
0.00 |
|
MRSA |
19 |
26 |
0.00 |
0.00 |
0.00 |
|
S. enterica ser. Typhimurium |
0 |
24 |
0.00 |
0.00 |
0.00 |
|
Klebsiella pneumoniae |
7 |
25 |
0.00 |
0.00 |
0.00 |
|
Escherichia coli |
20 |
31 |
0.00 |
0.00 |
0.00 |
|
Pseudomonas aeruginosa |
0 |
30 |
0.00 |
0.00 |
0.00 |
0.0 = No inhibition zone (Resistant)
|
|
|
Figure 4. Antimicrobial activity of 100 mg/ml ethanolic A. indica leaves extract against Bacillus cereus and MRSA |
|
|
|
Figure 5. Antimicrobial activity of 200 mg/ml and 500 mg/ml ethanolic A. indica leaves extract against Bacillus cereus. |
Different studies reported the presence of biologically active compounds in A. indica leaves extracts at different wave lengths. HPLC analysis of methanol and acetone/water extracts of A. indica leaves at 254 nm was carried out by Biney et al. (2020). Methanol extract of A. indica exhibited higher content of phytochemical compounds (alkaloids, flavonoids, and phenols) at a concentration of 0.1 mg/ml compared to the acetone/water extract (Lutfiyati et al., 2022; Sabar et al., 2022). HPLC analysis conducted also reveals seven peaks for methanol extract and six for acetone/water extract with different heights. The methanolic extract of A. indica leaves possessed strong antibacterial activity against different types of bacteria. GC-MS analysis revealed the presence of 30 chemical compounds, including fatty acids (11), hydrocarbons (9), pyridine derivatives (2), aldehydes (2), phenol group (1), aromatic substances (1), coumarins (1), and monoterpenes (1). In silico and in vitro tools revealed that beta. d-Mannofuranoside, O-geranyl was the most active compound on different bacterial proteins and it passed 5 rules of drug-likeness properties (Altayb et al., 2022).
Another study reported that the ethanolic extract of A. indica leaves has in phytochemical composition many compounds of the flavonoid class, and quercetin is its major compound. Chlorogenic acid and gallic acid were also detected (De Sousa Júnior et al., 2018). Findings of Falana and Nurudeen, (2020) showed a strong occurrence of antimicrobial compounds (tannin, alkaloid, steroid, saponin, and anthraquinone) in acetone, hexane, and ethyl acetate extracts of A. indica. Negative antimicrobial results of aqueous A. indica extract do not mean the absence of bioactive constituents. Parekh and Chanda, (2007) reported that traditional healers use primarily water for extraction but plant extracts from organic solvents have been found to give more consistent antimicrobial activity compared to water extracts.
According to Sakakibara et al. (2003), simple phenols were eluted at the retention time between 5.8 and 34.3 min, catechins at 8.1 and 26.1 min, anthocyanins between 17.4 and 47.7 min, flavones, flavonols, isoflavones and flavanones in the form of glycosides were eluted between 20.1 and 61.4 and aglycons at retention time between 26.7 and 91.6 min. HPLC analysis of phenolic compounds in A. indica methanolic extract was done at 254 nm. Sixteen peaks were seen in different retention times from 0.491 to 27.433 min. Simple polyphenols were eluted at a retention time of 6.033 min, catechins at 8.617, 9.058, 9.500, and 9.675min. Glycosides form of flavones, flavonols, isoflavones, and flavanones were seen at retention times 22.725, 24.033, and 24.158 min. At the retention time of 26.992 and 27.433 min, aglycons were eluted. According to a previous study, it was suggested that the longer peaks in A. indica extracts at retention time between 8.667 and 8.896 min could be either simple phenols or catechins (Supritha & Radha, 2018).
These findings were supported by the previous research results from Santosh Medical College and Hospital in India, which studied the antibacterial potential of A. indica extract against Gram-negative uropathogens. Ethanolic A. indica leaves extract were observed to inhibit the growth of all tested pathogenic bacteria. Acinetobacter baumannii was the most sensitive among all isolates (Faujdar et al., 2020).
In another study, A. indica methanolic and petroleum ether leaves extracts were tested against selected pathogens by researchers from Sudan International University. Staphylococcus aureus and Methicillin-resistant Staphylococcus aureus were the only bacteria susceptible to A. indica extracts. For methanolic extract, the zone of inhibition at 75% concentration was 12.0 mm for S. aureus and 11.0 mm for MRSA. For petroleum ether extract, the zone of inhibition at 75% concentration was 14.0 mm for S. aureus and 17.0 mm for MRSA. The result obtained indicated that A. indica leaves extracts have enormous antibacterial effects and may be exploited for the treatment of various infectious diseases (Fasher Bory et al., 2021).
The methanolic extract of A. indica leaves showed the highest antibacterial activity in comparison to the aqueous A. indica leaves extract. It was concluded that the presence of biologically active compounds in A. indica plant extract could be affected by the solvent used in extraction (Ibrahim & Kebede, 2020). In contrast, aqueous A. indica leaves and bark extract showed good antibacterial potential against Vibrio cholera and Bacillus subtilis with a zone of inhibition of 17 mm for each of them. E. coli and S. typhi were less susceptible to A. indica aqueous extract (Raut et al., 2014). These results support the data recorded in current study.
For MRSA the highest zone size was found at 16.4 mm with ethanolic extract at 200 mg/ml conc. When compared with methanolic extract at the same conc., the zone size was reduced to 15.3 mm. The same was observed for other Gram-positive bacteria indicating that ethanol was the best solvent for Neem plant extract against these bacteria. In contrast, when Neem leaves extracts were tested against Gram-negative P. aeruginosa, the maximum zone size was found 21.2 mm at 200 mg/ml methanolic extract which is significantly different from the zone size of the same conc. of ethanolic extract as well.
Conclusion
This study showed that A. indica leaves extracts have antibacterial potential against both Gram-positive and Gram-negative bacteria. For Gram-positive bacteria, ethanolic extract gives the best antimicrobial results compared to other extracts. Three Gram-negative bacteria; Klebsiella pneumoniae, Escherichia coli, and S. enterica ser. Typhimurium was resistant to all A. indica leaves extracts. Both ethanolic and methanolic extracts showed antimicrobial effects on Pseudomonas aeruginosa with more sensitivity for methanolic extract. Negative results were found for aqueous extract with all tested bacteria indicating the resistance of pathogenic bacteria. HPLC results indicated that the presence of phenolic compounds in A. indica leaves extracts made it a strong antimicrobial agent and these phenolic compounds could be a great source in future drug development projects.
Acknowledgments: Our acknowledgment to King Fahad Medical Research Center (KFMRC), King Abdulaziz University, Jeddah, Saudi Arabia for providing all the facilities for experimental research work.
Conflict of interest: None
Financial support: None
Ethics statement: None
Adlan, A. H., Alobaid, A., El Nima, E. I., Waggiallah, H. A., & Eltayeb, L. B. (2021). Antimicrobial susceptibility pattern for community-acquired uro-pathogens among UTI geriatric patients. International Journal of Pharmaceutical Research & Allied Sciences, 10(1), 24-33.
Al-Ghamdi, M., Aly, M. M., & Sheshtawi, R. M. (2020). Antimicrobial activities of different novel chitosan-collagen nanocomposite films against some bacterial pathogens. International Journal of Pharmaceutical and Phytopharmacological Research, 10(1), 114-121.
Altayb, H. N., Yassin, N. F., Hosawi, S., & Kazmi, I. (2022). In-vitro and in-silico antibacterial activity of Azadirachta indica (Neem), methanolic extract, and identification of Beta. d-Mannofuranoside as a promising antibacterial agent. BMC Plant Biology, 22(1), 262. doi:10.1186/s12870-022-03650-5
Alves, P. D., Brandão, M. G. L., Nunan, E. A., & Vianna-Soares, C. D. (2009). Chromatographic evaluation and antimicrobial activity of Neem (Azadirachta indica A. Juss., Meliaceae) leaves hydroalcoholic extracts. Brazilian Journal of Pharmacognosy, 19(2B), 510-515.
Andersson, D. I., & Hughes, D. (2011). Persistence of antibiotic resistance in bacterial populations. FEMS Microbiology Reviews, 35(5), 901-911. doi:10.1111/j.1574-6976.2011.00289.x
Assaggaf, H. M. (2021). Antimicrobial effects of the laundering process applied to household linens in the hotels of Makkah city. International Journal of Pharmaceutical Research & Allied Sciences, 10(3), 64-69.
Biney, E. E., Nkoom, M., Darkwah, W. K., & Puplampu, J. B. (2020). High-performance liquid chromatography analysis and antioxidant activities of extract of Azadirachta indica (Neem) leave. Pharmacognosy Research, 12(1), 29-34. doi:10.4103/pr.pr_14_19
De Sousa Júnior, D. L., Cordeiro, P. P. M., de Sousa Silveira, Z., Macêdo, N. S., Boligon, A. A., dos Santos, J. F. S., da Costa, J. G. M., & da Cunha, F. A. B. (2018). Phytochemical profile of leaves extract of Azadirachta indica A. Juss and toxicity against Drosophila melanogaster. Proceedings of MOL2NET 2018, International Conference on Multidisciplinary Sciences, 4th Edition, 5557. doi:10.3390/mol2net-04-05557
Deisy, D., Aditama, L., & Yulia, R. (2023). Consumers’ knowledge, attitude and practice of respiratory symptoms self-medication in community pharmacy during COVID-19 pandemic. Journal of Advanced Pharmacy Education and Research, 13(1), 66-72. doi:10.51847/kzJZAdVcE5
El-Sokkary, M. M. A. (2023). Molecular detection of some Gram-negative bacterial species using folp gene sequences. Journal of Advanced Pharmacy Education and Research, 13(1), 35-41. doi:10.51847/2B4jrAeFDF
Falana, M. B., & Nurudeen, Q. O. (2020). Analysis of secondary metabolites and in vitro evaluation of extracts of Carica papaya and Azadirachta indica leaves on selected human pathogens. Notulae Scientia Biologicae, 12(1), 57-73. doi:10.15835/nsb12110541
Fasher Bory, W. O., Hammad, M. A., & Idris, A. A. (2021). Evaluation of in vitro antimicrobial effects of Azadirachta indica (Neem) leaves extracts against selected pathogens. Microbes and Infectious Diseases, 3(3), 744-750. doi:10.21608/mid.2021.109886.1213
Faujdar, S. S., Bisht, D., & Sharma, A. (2020). Antibacterial potential of Neem (Azadirachta indica) against uropathogens producing beta-lactamase enzymes: A clue to a future antibacterial agent? Biomedical and Biotechnology Research Journal, 4(3), 232-238. doi:10.4103/bbrj.bbrj_38_20
Feghhi, M., Moghimi, M. A., Kasiri, A., & Farrahi, F. (2023). Relative frequency of inherited retinal disorders in Khuzestan province, southern Iran. Journal of Advanced Pharmacy Education and Research, 13(1), 42-45. doi:10.51847/EU0Ov98OOe
Fernandes, S. R., Barreiros, L., Oliveira, R. F., Cruz, A., Prudêncio, C., Oliveira, A. I., Pinho, C., Santos, N., & Morgado, J. (2019). Chemistry, bioactivities, extraction and analysis of azadirachtin: State-of-the-art. Fitoterapia, 134, 141-150. doi:10.1016/j.fitote.2019.02.006
Gofur, N. R. P., Gofur, A. R. P., Putri, H. M., Soesilaningtyas, S., Halimah, A. N., Feriana, D., Rusdiana, E., Wahjuni, S., Rosa, M. L. L., & Yusof, Z. Y. B. M. (2023). Drug choice to lowering risk contiguity with Morbus Hansen disease: a review article. Journal of Advanced Pharmacy Education and Research, 13(1), 73-79. doi:10.51847/CksXmT6VSy
Gupta, S. C., Prasad, S., Tyagi, A. K., Kunnumakkara, A. B., & Aggarwal, B. B. (2017). Neem (Azadirachta indica): An Indian traditional panacea with a modern molecular basis. Phytomedicine, 34, 14-20. doi:10.1016/j.phymed.2017.07.001
Ibrahim, N., & Kebede, A. (2020). In vitro antibacterial activities of methanol and aqueous leave extracts of selected medicinal plants against human pathogenic bacteria. Saudi Journal of Biological Sciences, 27(9), 2261-2268. doi:10.1016/j.sjbs.2020.06.047
Iwu-Jaja, C. J., Jaca, A., Jaja, I. F., Jordan, P., Bhengu, P., Iwu, C. D., Okeibunor, J., Karamagi, H., Tumusiime, P., Fuller, W., et al. (2021). Preventing and managing antimicrobial resistance in the African region: A scoping review protocol. Plos One, 16(7), e0254737. doi:10.1371/journal.pone.0254737
Khursheed, A., & Jain, V. (2021). Phytochemical screening, antioxidant, and antimicrobial activity of different Portulaca oleracea L. extract growing in Kashmir valley. Journal of Biochemical Technology, 12(3), 1-8.
Kumar, V. S., & Navaratnam, V. (2013). Neem (Azadirachta indica): Prehistory to contemporary medicinal uses to humankind. Asian Pacific Journal of Tropical Biomedicine, 3(7), 505-514. doi:10.1016/S2221-1691(13)60105-7
Lutfiyati, H., Yasin, N. M., Thobari, J. A., & Ikawati, Z. (2022). The implementation of antimicrobial stewardship in Indonesia: a regional survey in hospitals. Journal of Advanced Pharmacy Education and Research, 12(4), 19-26. doi:10.51847/d6u4SIWaYj
Matos de Opitz, C. L., & Sass, P. (2020). Tackling antimicrobial resistance by exploring new mechanisms of antibiotic action. Future Microbiology, 15(9), 703-708.
Mohankumar, J. B., Uthira, L., & Maheshwari, S. U. (2020). Total phenolic content of organic and conventionally grown gourd vegetables. Journal of Science and Technology, 5(4), 166-172. doi:10.46243/jst.2020.v5.i4.pp166-172
Nalawade, T. M., Bhat, K. G., & Sogi, S. (2016). Antimicrobial activity of endodontic medicaments and vehicles using agar well diffusion method on facultative and obligate anaerobes. International Journal of Clinical Pediatric Dentistry, 9(4), 335-341. doi:10.5005/jp-journals-10005-1388
Nurcahyo, H., Febriyanti, R., Riyanta, A. B., Sutanto, H., & Herdwiani, W. (2023). The influence of extraction temperature and time on antiradical activity and total phenolic extract of Ceciwis. Journal of Advanced Pharmacy Education and Research, 13(1), 31-34. doi:10.51847/nQYMC4fZCL
Parekh, J., & Chanda, S. (2007). Antibacterial and phytochemical studies on twelve species of Indian medicinal plants. African Journal of Biomedical Research, 10(2), 175-181.
Rahayuningtyas, E. D., Sufiawati, I., Lesmana, R., & Nur, M. (2022). Cytotoxicity effect of ozone in oral squamous cell carcinoma: an in vitro study. Journal of Advanced Pharmacy Education and Research, 12(4), 6-11. doi:10.51847/Qma6bNB6vL
Raut, R. R., Sawant, A. R., & Jamge, B. B. (2014). Antimicrobial activity of Azadirachta indica (Neem) against pathogenic microorganisms. Journal of Academia and Industrial Research, 3(7), 327-329.
Ren-Zhang, L., Chee-Lan, L., & Hui-Yin, Y. (2020). The awareness and perception on antimicrobial stewardship among healthcare professionals in a tertiary teaching hospital Malaysia. Archives of Pharmacy Practice, 11(2), 50-59.
Sabar, M. H., Jaafar, I. S., & Radhi, A. A. (2022). Factors controlling development of benazepril mouth dissolving drug delivery system. Journal of Advanced Pharmacy Education and Research, 12(4), 12-18. doi:10.51847/JQC55C3x8x
Sakakibara, H., Honda, Y., Nakagawa, S., Ashida, H., & Kanazawa, K. (2003). Simultaneous determination of all polyphenols in vegetables, fruits, and teas. Journal of Agricultural and Food Chemistry, 51(3), 571-581. doi:10.1021/jf020926l
Shahveh, M., Tajbakhsh, E., Momtaz, H., & Ranjbar, R. (2020). Antimicrobial resistance, biofilm formation, and virulence factors in Enterococcus faecalis strains isolated from urinary tract infection in Kermanshah, Iran. Archives of Pharmacy Practice, 11(3), 79-88.
Supritha, P., & Radha, K. V. (2018). Estimation of phenolic compounds present in the plant extracts using high pressure liquid chromatography, antioxidant properties, and antibacterial activity. Indian Journal of Pharmaceutical Education and Research, 52(2), 321-326.
Tacconelli, E., Carrara, E., Savoldi, A., Harbarth, S., Mendelson, M., Monnet, D. L., Pulcini, C., Kahlmeter, G., Kluytmans, J., Carmeli, Y., et al. (2018). Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. The Lancet Infectious Diseases, 18(3), 318-327. doi:10.1016/S1473-3099(17)30753-3
Tawfik, D. I., Elkhashab, D. M., Elnour, R. K. A., Kamal, N. M., Khorshid, O. A., & Mehesen, M. N. (2023). Possible renoprotective effect of valsartan/sacubitril versus valsartan and Metformin in rat model of diabetic nephropathy. Journal of Advanced Pharmacy Education and Research, 13(1), 51-61. doi:10.51847/VZXo7OkKpr
Tiwari, R., Sandil, S., Nain, P., & Kaur, J. (2020). Bacteriological analysis with antimicrobial sensitivity and resistance pattern in blood culture of septicemic patient from different wards of a tertiary care hospital in India. International Journal of Pharmaceutical and Phytopharmacological Research, 10(4), 112-119.
Uzzaman, S. (2020). Pharmacological activities of Neem (Azadirachta indica): A review. International Journal of Pharmacognosy and Life Science,1(1),38-41. doi:10.33545/27072827.2020.v1.i1a.8
World Health Organization. (2014). Antimicrobial resistance: global report on surveillance. World Health Organization. URL: https://apps.who.int/iris/bitstream/handle/10665/112642/?sequence=1