
Study of the Features of Choledocholithiasis in Elderly Patients
Almohamad Almahmud Tamim, Alexey Klimov*
Abstract
Introduction: Choledocholithiasis occurs most commonly, the probability of calculi in the bile duct increases significantly with the age of patients. Our study aimed to assess the situation of choledocholithiasis in Moscow, and study the characteristics of the disease in elderly patients. Methods: This was a retrospective study, including patients referred to the surgical department of the V. V. Vinogradov state medical center in Moscow, for the periods between 2017 - 2019. Data were collected from the records of the patients and cross-checked with endoscopic and cholangiography images. A total of 140 patients were included in this study. Results: The mean age of the patients was 79.9 years. Patients presented with obstructive jaundice (58.57%), cholangitis (25%), biliary colic or upper abdominal pain (14.22%), and acute biliary pancreatitis (2.14%). There were 15 (10.71%) post-cholecystectomy patients. Concomitant gallbladder stones were found in 95 patients (67.85%). Juxta-papillary diverticula were found in 19 patients (13.57%). Seven patients (5%) and 15 patients (10.71%) were found to have common bile duct strictures and choledochal cysts, respectively. Stones were commonly found in the distal common bile duct (68.57%). A majority of the patients had a single stone (47.85%). In 115 patients (82.14%), the size of the largest stones measured between 0.5-1.5 cm. Conclusion: Choledocholithiasis affects the elderly ages of most patients, the percentage of its occurrence has increased in females compared to that of males. The most common symptoms of the disease were obstructive jaundice, with the formation of distal stones, with no primary formation being. These characteristics were favorable for successful endoscopic removal of stones.
Keywords: Choledocholithiasis, common bile duct, distribution, elderly, features.
Introduction
Common bile duct (CBD) stones are crystallized deposits containing cholesterol and /or bilirubin, which are most often formed in the gallbladder (Tiderington et al., 2016). CBD commonly occurs in about 20% of adults in Europe and the USA, it’s prevalence rate around the world varies depending on the environment and the genetic factors of people (Portincasa, Moschetta, and Palasciano 2006) .
Currently, cholecystectomy is the most effective way in the treatment of cholelithiasis, it was recorded that more than 700 thousand cholecystectomies performed in the United States and up to 300 thousand in the Russian Federation annually (Ermolov et al. 2002). The probability of calculi in the bile duct increases significantly with the age of patients, Choledocholithiasis in patients under the age of 60 years old observed on average in 6% of cases, while in patients older than 80 years - up to 33% and higher. Naturally, calculous cholecystitis complicated by obstructive jaundice reaches 44.0-83.9% of patients (Dorrance et al. 1999; Targarona et al. 1996).
CBD stones are classified as primary and secondary stones, a stone formed in the CBD is considered as a primary stone, whereas gallstones can thread from the gallbladder and through the cystic duct, to the common bile duct (CBD) spontaneously (Jones and Deppen 2020). These stones are known as secondary bile duct stones (Frybova et al. 2018; Wilkins et al. 2017).
Approximately, one-third of patients have a spontaneous passage of stones along the bile ducts, based on the disappearance of stones 6 weeks after the diagnosis is determined using an in-situ catheters of cholangiography (Maple et al. 2010). In general, patients with symptomatic bile duct stones are mostly at greater risk of future problems than patients with asymptomatic stones. The most common symptoms in a patient with gallstones are pain in the right hypochondrium and/or epigastrium, nausea, and vomiting (Ren-Zhang, et al., 2020; Alzahrani, et al., 2019; Darkhor, et al., 2018; Mathialagan, et al., 2018). The pain usually lasts longer than with biliary colic. Patients may also complain of intermittent jaundice, if the bile stone is large enough and in the correct position, complete obstruction of the bile duct may occur, and patient jaundice can persist and progress. A thorough analysis of the symptoms may indicate that the patient has colorless stools and dark urine as a result of conjugated hyperbilirubinemia. If the stone passes through the CBD and then blocks the pancreatic duct and acute pancreatitis may occur (Jaffe 2009; Sanders and Kingsnorth, 2007).
Our study aimed to assess the epidemiological situation of choledocholithiasis in Moscow, and study some clinical and endoscopic features in elderly patients.
Materials and Methods
This was a retrospective study including patients referred to the surgical department of the V. V. Vinogradov state medical center in Moscow- Russia, for endoscopic management of CBD stones from all parts of the city. All patients who underwent therapeutic ERCP for choledocholithiasis for the first time for the period from 2017 to 2019 were included in the study. All patients met the standard to be classified into the high-risk group of having CBD stone in proportion to the American Society of Gastrointestinal Endoscopy guidelines (Maple et al. 2010). Patients who underwent ERCP as a planned second or subsequent time and patients who were not found to have CBD stone during ERCP were excluded.
Patients were selected from the surgical department database of the City clinical hospital named after. V. V. Vinogradova in Moscow- Russia. Data were collected from the records of the patients and cross-checked with endoscopic and cholangiography images. A proforma containing demographic, clinical, ultrasound scan (USS), and ERCP data for each patient was prepared. Information was recorded on the amount and size of the stones, their position in the biliary tree, CBD dimensions. If multiple stones were found, it was considered the size of the largest stone. For the analysis, the results of cholangiogram were considered over USS results. Data were analyzed using (Microsoft Excel 2016) and the statistical program StatPlus v.5. According to the age, the patients have grouped into 60-64, 65-69, 70-74,75-79,80-93, and ≥ 94 year’s categories.
Results
Only 140 patients had sufficient data for analysis out of 199 patients diagnosed with choledocholithiasis by ERCP. The mean age of the selected inhabitants in this research was 79.9 years old (range 60-94 years). The most common age range was 80-93 years (47.85%) (Fig. 1). The ratio of male: female was 40.7:59.3. The mean age for males was 89 years (SD±1.860), and for females was 80 years (SD±1.540). A significant difference (p<0.001) was recorded between the mean ages of the patients.
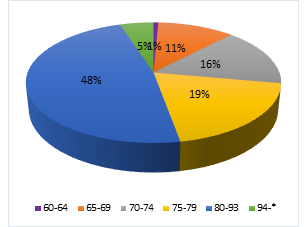
Figure 1. Age distribution of patients with choledocholithiasis
Patient distribution according to the clinical symptoms is depicted in Table 1. A significant increase (p<0.01) was recorded in the average age of patients with cholangitis compared to patients with acute biliary pancreatitis or abdominal pain/biliary colic. During ERCP, about 83.57% of patients with cholecystitis were diagnosed with acute septicemia. Out of 20 patients with upper abdominal pain or biliary colic, 12 patients (8.57%) were registered for cholecystectomy due to cholelithiasis, and the ERCP was performed before the surgery.
Table 1. Patient distribution according to the clinical symptoms
|
Clinical symptoms |
Total |
Mean age (years) |
Males |
Females |
|
Obstructivejaundice |
82 (58.57%) |
85.5 |
28 (34.14%) |
54 (65.85%) |
|
Cholangitis |
35 (25%) |
89.7 |
21 (60%) |
14 (40%) |
|
Abdominal pain/Biliary colic |
20 (14.28%) |
81.4 |
8 (40%) |
12 (60%) |
|
Biliary pancreatitis |
3 (2.14%) |
79.2 |
0 (0%) |
3 (100%) |
During the research period, cholecystectomy was performed for 15 patients (10.71%), of the remaining 125 patients with an intact gallbladder, 95 patients (67.85%) were diagnosed with gallbladder stone. No relationship was observed between gender, age, clinical symptoms, and the presence of gallstones.
CBD strictures were found in 7 patients (5%), and choledochal cysts in 15 patients (10.71%). 19 patients (13.57%) were found to have a juxtapapillary diverticulum. Patients with diverticula (mean age 74.7 years) were significantly older than patients without them (mean age 67.2 years, p<0.005), and they were significantly more possible to have multiple stones and to present with jaundice than other studied complications of the disease (p<0.01).
Table 2 shows the distribution of patients according to features of the stones (the number of stones, size, and position of them in the biliary tree).
Table 2. The distribution of patients according to the features of the stones.
|
Classification |
According to stone amount |
According to position of the stone |
According to size of the stone |
|||||||||
|
Single stone |
2 stones |
3 stones |
Multiple stones |
Intrahepatic |
Proximal |
Mid |
Distal |
< 0.5 cm |
0.5-1 cm |
1-1.5 cm |
> 1.5 cm |
|
|
Number of patients |
67 |
15 |
5 |
53 |
1 |
9 |
34 |
96 |
18 |
47 |
68 |
7 |
|
% |
47.85 |
10.71 |
3.57 |
37.85 |
0.71 |
6.42 |
24.28 |
68.57 |
12.85 |
33.57 |
48.57 |
5 |
Discussion
Most of the patients in this study (85.71%) were found to have obstructive jaundice, cholangitis, or acute biliary pancreatitis, and these are considered serious complications of the disease in older patients, while the rest of the study patients had either distinct biliary colic or presented with non-specific upper abdominal pain, which indicates the symptoms of a distinct choledocholithiasis. Since patients included in the sample originated from various parts of Moscow city, the findings can be generalized to the Moscow population. Therefore, this study characterizes the disease features of a unique population.
The increase in age and male gender are considered as risk factors for complicated choledocholithiasis (Kummerow et al. 2012). In our study, it was found that choledocholithiasis affects the elderly population with a predominance of women. The mean age for females with this disease in this study was less than the mean age for males by 9 years, this indicates that females to be at increased risk for symptomatic choledocholithiasis.
The older patients presented an inclination to have cholangitis while the younger patients showed an inclination to have abdominal pain or biliary colic, so confirming the fact that older patients had a more complicated disease.
Juxtapapillary diverticulum is associated with choledocholithiasis, which leads to technical difficulty during biliary cannulation (Jones and Deppen 2019). The lower spread of juxtapapillary diverticulum was recorded in the patients of our study (13.57%), compared to the other studies reported a spread of 26% (Hagege et al. 1992). Based on the present information, a higher spread of diverticula in older patients proposes an acquired etiology. (Osnes et al. 1981) Choledochal cysts and CBD strictures are considered important factors that help to facilitate the formation of stones (Savader et al. 1991), though, in this study, only 10.71% and 5 % of the patients were with choledochal cysts and CBD stricture, respectively.
The characteristics of stones help predict the outcome of endoscopic clearance. Big, impacted, multiple or intrahepatic stones are considered difficult to extract and need more advanced techniques (McHenry and Lehman 2006; Stefanidis et al. 2012). Most of the patients in this study had single or distal CBD stones, the removal of which is not a complicated mission. Furthermore, 94.99% of patients had stones smaller than 1.5 cm, which is also a suitable feature for successful endoscopic removal (McHenry and Lehman 2006).
The standard to classify CBD stones into primary or secondary stones were presented by (Madden 1973) then modified by (Saharia, Zuidema, and Cameron 1977), they identified CBD stones as “the absence of a long cystic duct remnant or a biliary stricture from the previous cholecystectomy, at least a two-year symptom-free interval following cholecystectomy, and soft, light brownstones or sludge present in the common duct”. Based on the previous classification, all patients with intact gallbladder (89.28%) were classified under secondary stone class. All the after-cholecystectomy patients (10.71%) were also classified under this class, where they showed symptoms within two years from the date of cholecystectomy.
CBD stones found in our study patients are mainly single, distal, and small, which are the suitable features for effective endoscopic removal.
Conclusions
As a result of our study, we conclude that choledocholithiasis affects the elderly ages of most patients who should be given more attention because they tend to follow a more complex disease course. The percentage of its occurrence has increased in females compared to that of males. Also, we found that the most common symptoms of the disease were obstructive jaundice, with the formation of distal stones, and with a high rate of single stones with a diameter of 0.5-1.1 cm, with no primary formation being. These characteristics were favorable for successful endoscopic removal of stones. None of the stones found in our study may be classified into a primary CBD stone according to the available standards, although a lot of the stones were found in an anatomically normal biliary tree. As a result, it is necessary to review the classification theory of CBD stones.
Abbreviations
CBD: Common Bile Duct
ERCP: Endoscopic Retrograde Cholangiopancreatography
USS: Ultrasound scan.
References
Alzahrani, M. I., Alzahrani, M. I., Alsolami, E. A., Al Sulami, A. H., Abdulrahman, A., Alhejaili, M. A. A., ... & Ahmed, Z. (2019). Evaluative Role of Family Physician in Diagnosis and Management of Gout in Primary Health Care Centers: A Simple Literature Review. Archives of Pharmacy Practice, 10(3), 126-129.
Darkhor, S., Estebsari, F., Hosseini, M., Charati, J. Y., & Vasli, P. (2018). Effect of health promotion intervention on Nurses’ healthy lifestyle and health-promoting behaviors: RCT study. Journal of Advanced Pharmacy Education & Research, 8(1), 108-114.
Dorrance HR, Lingam MK, Hair A, Oien K, O’Dwyer PJ. (1999). Acquired Abnormalities of the Biliary Tract from Chronic Gallstone Disease. Journal of the American College of Surgeons, 189(3): 269–73. Available from: http://dx.doi.org/10.1016/s1072-7515(99)00126-x
Ermolov AS, Dasaev NA, Iurchenko SV, Durgarian TV, Riabykh VI. (2002). Diagnosis and Treatment of Cholangiolithiasis after Cholecystectomy. Surgery journal, 4: 4–10. Available from: https://pubmed.ncbi.nlm.nih.gov/12001681/
Frybova B, Drabek J, Lochmannova J, Douda L, Hlava S, Zemkova D, Mixa V, Kyncl M, Zeman L, Rygl M, Keil R. (2018). Cholelithiasis and Choledocholithiasis in Children; Risk Factors for Development. PLoS ONE, 13(5). Available from: http://dx.doi.org/10.1371/journal.pone.0196475
Hagège H, Berson A, Pelletier G, Fritsch J, Choury A, Liguory C, Etienne JP. (1992). Association of Juxtapapillary Diverticula with Choledocholithiasis but Not with Cholecystolithiasis. Endoscopy, 24(4): 248–51. Available from: http://dx.doi.org/10.1055/s-2007-1010476
Jaffe, Philip E. (2010). Biliary Colic. Decision Making in Medicine: An Algorithmic Approach: Third Edition: 194–95. Available from: http://dx.doi.org/10.1016/b978-0-323-04107-2.50073-9
Jones, Mark W., and Jeffrey G. Deppen. (2020). StatPearls Physiology, Gallbladder. http://www.ncbi.nlm.nih.gov/pubmed/29494095. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482488/
Kummerow KL, Shelton J, Phillips S, Holzman MD, Nealon W, Beck W, Sharp K, Poulose BK. (2012). Predicting Complicated Choledocholithiasis. Journal of Surgical Research, 177(1): 70–74. Available from: http://dx.doi.org/10.1016/j.jss.2012.04.034
Madden, J. L. (1973). Common Duct Stones. Their Origin and Surgical Management. Surgical Clinics of North America, 53(5): 1095–1113. Available from: http://dx.doi.org/10.1016/s0039-6109(16)40139-8
Maple JT, Ben-Menachem T, Anderson MA, Appalaneni V, Banerjee S, Cash BD, Fisher L, Harrison ME, Fanelli RD, Fukami N, Ikenberry SO, Jain R, Khan K, Krinsky ML, Strohmeyer L, Dominitz JA. (2010). The Role of Endoscopy in the Evaluation of Suspected Choledocholithiasis. Gastrointestinal Endoscopy, 71(1): 1–9. Available from: http://dx.doi.org/10.1016/j.gie.2009.09.041
Mathialagan, A. G., JA, J. A., Dinesh, M., Azra, N., Selvaganapathi, G., Harikrishnan, T., ... & Vikneswaran, S. (2018). Patient attitudes and health information features as predictors of health promotion in Malaysia. Journal of Advanced Pharmacy Education & Research, 8(2), 43-48.
McHenry, Lee, and Glen Lehman. (2006). Difficult Bile Duct Stones. Current Treatment Options in Gastroenterology, 9(2): 123–32. Available from: http://dx.doi.org/10.1007/s11938-006-0031-6
Osnes, M, T Løotveit, S Larsen, and S Aune. (1981). Duodenal Diverticula and Their Relationship to Age, Sex, and Biliary Calculi. Scandinavian journal of gastroenterology, 16(1): 103–7. http://www.ncbi.nlm.nih.gov/pubmed/7233076 (May 5, 2020). Available from: http://www.ncbi.nlm.nih.gov/pubmed/7233076
Portincasa, Piero, Antonio Moschetta, and Giuseppe Palasciano. (2006). Cholesterol Gallstone Disease. Lancet, 368(9531): 230–39. Available from: http://dx.doi.org/10.1016/s0140-6736(06)69044-2
Ren-Zhang, L., Chee-Lan, L., & Hui-Yin, Y. (2020). The awareness and perception on Antimicrobial Stewardship among healthcare professionals in a tertiary teaching hospital Malaysia. Archives of Pharmacy Practice, 11(2), 50-59.
Saharia, P. C., Zuidema G. D., and Cameron J. L. (1977). Primary Common Duct Stones. Annals of Surgery, 185(5): 598–604. Available from: http://dx.doi.org/10.1097/00000658-197705000-00013
Sanders, Grant, and Andrew N. Kingsnorth. (2007). Gallstones. British Medical Journal, 335(7614): 295–99. Available from: http://dx.doi.org/10.1136/bmj.39267.452257.ad
Savader SJ, Benenati JF, Venbrux AC, Mitchell SE, Widlus DM, Cameron JL, Osterman FA Jr. (1991). Choledochal Cysts: Classification and Cholangiographic Appearance. American Journal of Roentgenology, 156(2): 327–31. Available from: http://dx.doi.org/10.2214/ajr.156.2.1898807
Stefanidis, G., C. Christodoulou, S. Manolakopoulos, and R. Chuttani. (2012). Endoscopic Extraction of Large Common Bile Duct Stones: A Review Article. World Journal of Gastrointestinal Endoscopy, 4(5): 167–79. Available from: http://dx.doi.org/10.4253/wjge.v4.i5.167
Targarona EM, Ayuso RM, Bordas JM, Ros E, Pros I, Martínez J, Terés J, Trías M. (1996). Randomized Trial of Endoscopic Sphincterotomy with Gallbladder Left in Situ versus Open Surgery for Common Bileduct Calculi in High-Risk Patients. Lancet (London, England), 347(9006): 926–29. http://www.ncbi.nlm.nih.gov/pubmed/8598755. Available from: http://dx.doi.org/10.1016/s0140-6736(96)91413-0
Tiderington, E., Lee, S. P., & Ko, C. W. (2016). Gallstones: new insights into an old story. F1000Research, 5. Available from: http://dx.doi.org/10.12688/f1000research.8874.1
Wilkins, Thad, Edward Agabin, Jason Varghese, and Asif Talukder. (2017). Gallbladder Dysfunction: Cholecystitis, Choledocholithiasis, Cholangitis, and Biliary Dyskinesia. Primary Care - Clinics in Office Practice, 44(4): 575–97. Available from: http://dx.doi.org/10.1016/j.pop.2017.07.002








