Prevalence of HDNF due to ABO, Rh (D) and Other Blood Groups among Newborns, Sudan
Abdel Rahim Mahmoud Muddathir, Elharam Ibrahim Abdallah, Wala Eldin Osman Elradi, Mohammed Elmobarak Elbasheir, Ream Elzain Abdelgadir, Hisham Ali Waggiallah*
Abstract
The determination of the frequency of HDFN found in jaundiced newborns in Sudan was the goal of the analysis. In Omdurman maternity inside a Sudanese hospital, 220 mothers and their babies who had jaundice altogether were received in hospital-Sudan and a prospective cross-sectional hospital-based analysis was carried out them. In addition to ABO and Rhesus blood group typing, indirect antiglobulin test (IAT) and direct coomb's test (DAT) was applied for mothers and their jaundiced newborns, respectively. IgG anti-A and anti-B were checked inside the infant’s plasma to detect any incompatibility of ABO. The infant’s blood samples were taken and it underwent the tests of Hemoglobin, Reticulocyte count, thin blood films, and packed cell volume to check the hemolytic status of the baby. The history of abortion, prophylactic anti-D and blood transfusion was written as well. From the analysis, 57.3% (63/110) was the fetus’s and newborn's frequency of hemolytic disease among the studied subjects. The ones with incompatibility of ABO are 28.6% (18/63), and the ones with incompatibility of Rh (D) are 20.6% (13/63) even while prophylactic anti-D was used, while 50.8% (32/63) as a result from other blood groups antigens. The study concluded that the most common cause of HDFN in the studied population is from the other blood group antigens. The analysis also showed that the happening of Rh (D) HDFN wasn’t erased in spite of the Rh immunoglobulin usage.
Keywords: ABO, Rh (D), Hemolytic disease of the fetus and newborn, Blood groups
Introduction
In 1609, a French midwife and her twins were considered as the first case received in HDN. In 1932, Diamond and his colleagues defined the word erythroblastosis fetalis, just as soon as they discovered there was a link in the circulation between jaundice, fetal hydrops, erythroblasts, and anemia (Myle & Al-Khattabi, 2021). In 1940, Landsteiner and Weiner found the Rh blood group system, and later on, Levine figured out the source of the disease. Chown found the pathogenesis of Rh alloimmunization to be due to hemorrhage which leads to the invasion of maternal circulation as a result of the passage of fetal RBCs carrying Rh positive antigen with a negative Rh antigen (Myle & Al-Khattabi, 2021; Rohmani et al., 2022).
In 1971, a recommendation was made by the World Health Organisation (WHO) that for every one mL of fetomaternal hemorrhage of Rh-positive packed RBCs or two mL of whole blood, a dose of 25 mcg (125 IU) of anti-D (IgG) immunoglobulin shall be administered intramuscularly, to stop the happening of HDN (Myle & Al-Khattabi, 2021). In 1998, the suggestion to include prophylaxis dose at 28 weeks gestation was reinforced by the American College of Obstetrics and Gynecologists and the American Association of Blood Banks (Pegoraro et al., 2020).
In a mother’s blood group O and fetuses blood group A or B, HND arises as a result of the incompatibility of ABO; spherocytosis is visible inside their peripheral blood film as well as a few erythroblasts, dissimilar to the incompatibility Rh (D), that possess a lot of erythroblasts (erythroblastosis fetalis) plus a small number of spherocytes (Hendrickson & Delaney, 2016). For the antibody screening that is carried out in most advanced countries, all pregnant women have a clear guideline, dissimilar to countries like Sudan, which is a developing country. According to what has been reported in the literature, alloimmunization frequency is widely varied from one area to another (Sperling et al., 2018; Webb & Delaney, 2018; Erickson, 2020; Li et al., 2020). All pregnant women, except for women who have a HDN history or women with a negative D antigen, may not be expected to undergo routine antibody screening because it may not be necessary (Moinuddin et al., 2019; Yang et al., 2019; Jallepalli et al., 2022; Zahid & Khan, 2022).
Published literature shows that there was no data available concerning HDN in Sudan. Therefore, the analysis made it a goal to round off the frequency of hemolytic disease of the fetus and newborn (HDFN) found in Sudanese newborns infected with jaundice.
Materials and Methods
It happened in a hospital in Sudan (Omdurman maternity hospital) and it is a study based on hospitals that was eventual and divisional. 110 newborn babies with jaundice and their 110 mothers took part in this investigation. A set of laboratory tests such as Direct coomb's test (DAT) for the jaundiced newborn and indirect antiglobulin test (IAT) for their mothers was carried out to confirm HDN, in addition to the identification of ABO and Rhesus (D) blood group types. By the use of indirect antiglobulin test, the existence of IgG anti-A and anti-B was examined to check for any incompatibility of ABO that may lead to ABO and HDN in babies, using A1, B, and O cells. Sysmex KX-21N was utilized in the measurement of Hb and PCV. To check red cells that are nucleated and spherocytes that show the hemolytic state and confirm the ABO HDFN, reticulocyte count and a thin blood film that is stained were executed (SIR John et al., 2011; Hendrickson & Delaney, 2016).
The measurement of reticulocyte count and overall serum bilirubin was executed. Additionally, the prophylactic anti-D, abortion, and blood transfusion records were collected, together with the mortality data of the newborns at the time which the testing period commenced. The 26th version of SPSS was utilized to study ANOVA, frequencies, and descriptive statistics tests. For an estimate equivalent to or below 0.05, the p-value is regarded, statistically, as significant.
Results and Discussion
110 newborn babies infected with jaundice and their 110 mothers altogether were accepted by the Omdurman maternity hospital. In (57.3%) 63/110 of the newborn babies and (42.7%) 47/110 of the mothers, the fetus and newborn's hemolytic disease frequency was observed with no traces of HDFN, based on the analysis results.
Regarding how frequent HDFN is among ABO, Rh (D), and other blood groups antigens, the percentage of newborns that were ABO incompatible with their mothers were 20%, the percentage of newborns with HDFN was 90% (18/20), and those without any traces of HDFN was 10% (2/20). In contrast, 15 of the newborns were Rh (D) incompatible with their mothers, 86.7% (13/15) of them had HDFN, and 13.3% (2/15) did not show the criteria of HDFN. Contrary to the previous analysis, the percentage of newborns with HDFN because of other blood group systems was 43.2% (32/74), whereas the ones without any traces of HDFN was 56.8% (42/74). It is shown in Table 1 below:
Table 1. frequency of HDFN among ABO, Rh (D), and other blood groups
|
HDFN |
ABO |
Rh (D) |
Other blood groups |
|
Positive |
18 (90%) |
13 (86.7%) |
32 (43.2%) |
|
Negative |
2 (10%) |
2 (13.3%) |
42 (56.8%) |
|
Total |
20 |
15 |
74 |
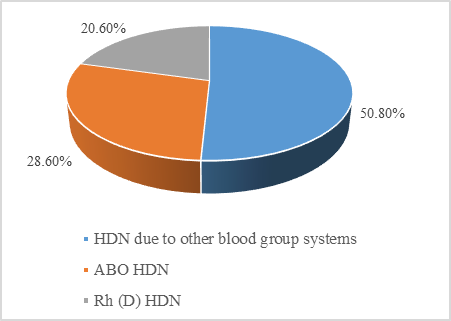
It was disclosed by the analysis of the overall net frequencies among the studied population that the percentage of newborns that had HDFN because of the incompatibility of Rh (D) was 20.6.% (13/63), the percentage of newborns that possessed ABO HDFN was 28.6% (18/63), and the percentage of those that had HDFN because of antigens of other blood groups was 50.8% (32/63). It is shown in Figure 1 below:
|
|
|
Figure 1. Frequency of Hemolytic disease of the fetus and newborn (HDFN) among the studied population |
Direct Antiglobulin Test results were positive in all newborns with Rh (D) and other blood groups HDN in addition to the positivity of the Indirect Antiglobulin Test among their mothers. In contrast, DAT showed positivity only in 38.9% (7/18) of the newborn who had ABO HDN, while the detection of the existence of IgG anti-B and anti-A in serum, by the checking of antibodies, was found positive in all of the instances.
Despite the apparent increase in the total serum bilirubin (13.3 mg/dl) and reticulocyte count (9.2%) in the newborns with ABO HDFN compared to HDFN due to Rh (D) (11.5 mg/dl) (8.2%) and HDFN due to other blood groups (12.1 mg/dl) (6.2%), there was no statistical difference obtained. P- value = 0.53, P-value = 0.12 respectively. Tables 2 and 3.
Table 2. Total serum bilirubin among different types of HDFN
|
Type of HDFN |
N |
Mean (mg/dl) |
STD |
Minimum (mg/dl) |
Maximum (mg/dl) |
P.vlue |
|
Rh (D) HDFN |
13 |
11.5 |
6.3 |
4.5 |
28.0 |
0.53 |
|
ABO HDFN |
18 |
13.3 |
5.0 |
6.1 |
23.6 |
|
|
Other blood group HDFN |
32 |
12.1 |
3.6 |
5.1 |
20.8 |
Table 3. Reticulocyte count among different types of HDFN
|
Type of HDFN |
N |
Mean (%) |
STD |
Minimum (%) |
Maximum (%) |
P-value |
|
Rh (D) HDFN |
13 |
8.2 |
4.0 |
2.0 |
14.0 |
0.12 |
|
ABO HDFN |
18 |
9.2 |
6.3 |
0.6 |
25.0 |
|
|
Other blood group HDFN |
32 |
6.2 |
4.5 |
0.2 |
25.0 |
O-B (O mothers, B baby) was shown by the mean total of serum bilirubin among ABO HDFN (TSB), to be higher than group O-A (O mothers, A baby), (15.6mg/dl) versus (13.6mg/dl) respectively [ The blood group O mothers gave birth to newborns with blood group B and they were 11 whereas 9 babies were from the blood group A].
38.5% (5/13) of the mothers that were Rh D negative had an abortion record without prophylactic anti-D. On the initial day of the last delivery, prophylactic anti D was administered to 46.2% (6/13). The dose was not standardized, which is unfortunate. 15.4% (2/13) were the remaining mothers and they did not have any record of abortion or blood transfusion. 63.2% (12/19) of those newborns were infected with HDFN and 17.3% (19/110) of the newborns with jaundice have died as shown by the mortality rate during the analysis time.
The investigation carried out on hemolytic disease of the fetus and newborns in Sudan wasn’t carried out accordingly and it wasn’t standardized; in diagnosing hemolytic disease of a newborn, most hospitals depend on the blood group incompatibility and result of DAT.
As a result of the lack of proper assessment for women that are pregnant and very limited antenatal care for those groups that are critical, HDFN is currently a big issue mainly in developing countries. Curing HDFN is more difficult than the prevention of HDFN. The early decision-making and attention that was given to this condition were reinforced by the availability of data about the distribution and frequency of HDFN, knowing the clues about the happenings and forms of HDFN was what this analysis targeted.
In Sudan, a large frequency of HDFN (57.3%), was revealed by the present analysis. Francesco Bennardello and Giuseppe Curciarello (2010) carried out an Italian study in which HDN was at hand in 55.5% of their surveyed group. Their study was following this frequency (Bennardello & Curciarello, 2013).
A diagnosis of ABO HDFN was made in (16.4%), in the current analysis; Bhat YR and Kumar CG, in 2012 (17.3%), agreed with this frequency to the Indian study (Routray et al., 2021) but when Feng CS, Wan CP, et al., who was from Hong Kong, found the incidence of ABO HDFN was 20% among infants with a serum bilirubin level of 300 mmols/L or more, it slightly reduced than frequency (Bi et al., 2019), and our results were slightly lower than this. It may be because their serum bilirubin concentration criteria was short. (0.7%) 1,456 / 203,384 of the newborns with ABO HDN were seen in an Italian analysis made by Francesco Bennardello and Giuseppe Curciarello (2010) as well (Bennardello & Curciarello, 2013).
O-A HDFN was less severe than O-B HDFN based on this study, and Kaplan M and Na'amad M agreed with these findings in their study, which supposed that: exchange blood transfusion could be the result of severe hemolysis and severe hemolysis could be caused by anti-B IgG (Ullah et al., 2016; Ansari et al., 2022). Additionally, YR and Kumar CG’s study was contradictory with it, which resulted to an equal incidence in severity being found between them (Routray et al., 2021).
Jeffrey Maisels' study agreed with our results when the positivity of DAT among ABO HDFN is put into consideration (Mitra & Rennie, 2017; Almuhanna et al., 2022), which found that: on the one-third of ABO HDFN, an antiglobulin test that was positive and direct was sensed.
Because of the Rh D antigen, HDFN was still existing, as the study showed. Nevertheless, prophylaxis IgG (D) immunoglobulin was utilized; our results are concordant with several previous studies (Bi et al., 2019; Erickson, 2020; Routray et al., 2021; Mobeen & Dawood, 2022). which may indicate improperly or shortage of immunoglobulin dose. In the last trimester, immunization with fetal RBCs might be carried out. Rh D-negative mothers, who were in their last trimester, were not given the prophylactic dose of anti D in most developing countries, and it must be taken as a guideline for all pregnant women that were Rh D-negative who had Rh D-positive husbands.
The present study demonstrated a high frequency of HDN due to other blood groups, and Bennardello and Giuseppe Curciarellos’ study was slightly lower this frequency; (94 / 203,384 cases HDN was due to other irregular antibodies) (Bennardello & Curciarello, 2013), the ethnic population difference in the studied population may be the cause of the contrast in the frequencies. Mortality data were recorded among the studied newborns, and it was agreed with the previous data of Nilgün A (Bennardello & Curciarello, 2013).
Limitation
Due to the high cost of providing an antibody identification panel, we could not identify the antibodies resulting from mother sera having HDNF due to other blood groups. More studies are needed to identify the type of antibodies in HDFN from other blood groups.
Conclusion
There was a high frequency of hemolytic disease of the fetus and newborns among the newborn babies infected with jaundice and the other blood groups are the cause of the most common type of HDFN, which is accompanied by ABO and Rh (D)
Acknowledgments: This Publication was supported by the Deanship of Scientific Research at Prince Sattam bin Abdulaziz University. The authors also thank Alzaiem Al-Azhari University staff members for their support. Many thanks to the Doctors and nurses at Omdurman maternity hospital who helped us by providing samples, patient data, and careful follow-up for the study.
Conflict of interest: None
Financial support: None
Ethics statement: The ethical review board of the Omdurman maternity hospital has accepted the investigation and the ethical clearance was gotten from the Medical laboratory college committee. Furthermore, before sample collection, written informed consent was obtained from all the newborns' parents.
Almuhanna, M. A., Alanazi, M. H., Ghamdi, R. N. A., Alwayli, N. S., Alghamdi, I. S. G., Qari, A. A., Alzahid, A. A., Alharbi, F. F., Alwagdani, N. M. A., & Alharthi, S. A. (2022). Tachycardia evaluation and its management approach, literature review. World Journal of Environmental Biosciences, 11(1), 4-8. doi:10.51847/7maH6sWjQy
Ansari, S., Alshamrani, B., Alzahrani, A., Alfayez, A., Alhebshan, N., & Alshamrani, A. (2022). Prevalence of dental fluorosis among teenagers; a cross-sectional study in the schools of Riyadh. Bulletin of Pioneering Researches of Medical and Clinical Science, 1(1), 13-17. doi:10.51847/37FuXGVEpm
Bennardello, F., & Curciarello, G. (2013). Survey on the prevention and incidence of haemolytic disease of the newborn in Italy. Blood Transfusion, 11(4), 518-527. doi:10.2450/2013.0179-12.
Bi, S. H., Jiang, L. L., Dai, L. Y., Zheng, H., Zhang, J., Wang, L. L., Wang, C., Jiang, Q., Liu, Y., Zhang, Y. L., et al. (2019). Rh-incompatible hemolytic disease of the newborn in Hefei. World Journal of Clinical Cases, 7(20), 3202-3207. doi:10.12998/wjcc.v7.i20.3202
Erickson, M. L. (2020). Alloimmunization in Pregnancy. In Immunologic Concepts in Transfusion Medicine (pp. 149-165). Elsevier.
Hendrickson, J. E., & Delaney, M. (2016). Hemolytic disease of the fetus and newborn: modern practice and future investigations. Transfusion Medicine Reviews, 30(4), 159-164. doi:10.1016/j.tmrv.2016.05.008
Jallepalli, V. R., Thalla, S., Gavini, S. B., Tella, J. D., Kanneganti, S., Yemineni, G., & Nadendla, R. R. (2022). Impact of patient education on quality of life in gastroesophageal reflux disease. International Journal of Pharmaceutical and Phytopharmacological Research, 12(1), 25-28. doi:10.51847/dAJecTWofD
Li, S., He, Z., Luo, Y., Ji, Y., Luo, G., Fang, Q., & Gao, Y. (2020). Distribution of maternal red cell antibodies and the risk of severe alloimmune haemolytic disease of the foetus in a Chinese population: a cohort study on prenatal management. BMC Pregnancy and Childbirth, 20(1), 1-11. doi:10.1186/s12884-020-03235-w
Mitra, S., & Rennie, J. (2017). Neonatal jaundice: aetiology, diagnosis and treatment. British Journal of Hospital Medicine, 78(12), 699-704. doi:10.12968/hmed.2017.78.12.699.
Mobeen, T., & Dawood, S. (2022). Studying the effect of perceived social support and mental health on marital burnout in infertile women. Journal of Integrative Nursing and Palliative Care, 3, 7-12. doi:10.51847/7DkM3Fkiu3
Moinuddin, I., Fletcher, C., & Millward, P. (2019). Prevalence and specificity of clinically significant red cell alloantibodies in pregnant women-a study from a tertiary care hospital in Southeast Michigan. Journal of Blood Medicine, 10, 283. doi:10.2147/JBM.S214118. eCollection 2019.
Myle, A. K., & Al-Khattabi, G. H. (2021). Hemolytic Disease of the Newborn: A Review of Current Trends and Prospects. Pediatric Health, Medicine and Therapeutics, 12, 491. doi:10.2147/PHMT.S327032
Pegoraro, V., Urbinati, D., Visser, G. H., Di Renzo, G. C., Zipursky, A., Stotler, B. A., & Spitalnik, S. L. (2020). Hemolytic disease of the fetus and newborn due to Rh (D) incompatibility: A preventable disease that still produces significant morbidity and mortality in children. PloS One, 15(7), e0235807. doi:10.1371/journal.pone.0235807
Rohmani, S., Desi, B. A., & Wardhani, W. D. (2022). Potassium-Azeloyl-Diglycinate BB-Cream formulation with Triethanolamine variation, and its effects on In-Vitro SPF stability and values. Journal of Advanced Pharmacy Education and Research, 12(1), 1-8. doi:10.51847/MUHp4ptold
Routray, S. S., Behera, R., Mallick, B., Acharya, D., Sahoo, J. P., Kanungo, G. N., & Pati, B. (2021). The spectrum of hemolytic disease of the newborn: evaluating the etiology of unconjugated hyperbilirubinemia among neonates pertinent to immunohematological workup. Cureus, 13(8). doi:10.7759/cureus.16940
SIR John V., Dacie S., & Lwis, S. M. (2011). Practical Haematology, 12th edition.
Sperling, J. D., Dahlke, J. D., Sutton, D., Gonzalez, J. M., & Chauhan, S. P. (2018). Prevention of RhD alloimmunization: a comparison of four national guidelines. American Journal of Perinatology, 35(02), 110-119. doi:10.1055/s-0037-1606609
Ullah, S., Rahman, K., & Hedayati, M. (2016). Hyperbilirubinemia in neonates: types, causes, clinical examinations, preventive measures and treatments: a narrative review article. Iranian Journal of Public Health, 45(5), 558.
Webb, J., & Delaney, M. (2018). Red blood cell alloimmunization in the pregnant patient. Transfusion Medicine Reviews, 32(4), 213-219. doi:10.1016/j.tmrv.2018.07.002
Yang, R., Li, G., He, X., & Ren, M. (2019). Analysis of neonatal hemolytic disease caused by Rh, MNS blood type system irregular antibodies [article in Chinese]. Journal of Clinical Haematology, 32(01), 109-12. doi:10.12998/wjcc.v7.i20.3202
Zahid, T. M., & Khan, N. S. (2022). Myrrh and chlorhexidine mouthwashes comparison for plaque, gingivitis and inflammation reduction: a 3-arm randomized controlled trial. Annals of Dental Specialty, 10(1), 39-46. doi:10.51847/ajwgutvUNV