
An update about Coronaviruses with Emphasis on Newly Emerged COVID 19
Lienda Bashier Eltayeb
Abstract
Coronaviruses (CoV) belong to enveloped single-stranded RNA viruses. Six COV namely HKU1, NL63, 229E, OC43, SARS, and MERS have been detected in humans, until December 2019 an outbreak of the novel coronavirus, known as “COVID-19/SARS-CoV-2”, in appeared Wuhan, China. As a consequence, life has changed dramatically and many people and health authorities are left confused about what they are to do to avoid dissemination of catastrophe. Even though much is identified about the mortality of the clinical phase of COVID 19 disease (symptoms ranging from the mild common cold to severe respiratory disease), but much less is understood about its pathophysiology. It has triggered infections and deaths more than SARS or MERS due to its high speed of transmission. Hence, SARS-CoV-2 is a considerable health and economic issue that can be horrific especially for immunocompromised or elderly people. In the last 18 years, we have been witness for the emergence of three extremely pathogenic zoonotic coronaviruses throughout history.
Key words: COVID 19, SARS-CoV-2, Coronavirus, Respiratory, Pandemic
Introduction
The 2019 novel coronavirus (2019-nCoV) or COVID-19 is an infectious disease caused by the most recently discovered coronavirus (SARS-CoV-2) (Lestari et al., 2020; Meconcelli et al., 2020). This new virus and disease were unknown before the outbreak began in Wuhan, China, since December 2019, which triggered an outbreak that flesh global attention because the virus was rapidly disseminated all over the world (Alshammari, 2020; Mohammadzadehgodini, 2020 ).
At least 830 cases were confirmed in nine countries as of 24 January 2020: China, Thailand, Japan, South Korea, Singapore, Vietnam, Taiwan, Nepal, and the United States, among which there had been twenty-six fatal accidents, mostly in patients with a massive form of the disease. While many details of this newly emerged virus including its source and its ability to transmit among humans remain unclear, an increasing number of cases also seem to have been the result of human-to-human transmission. Globally, as of 29 June 2020, there has been 10,294,019 confirmed cases of COVID 19, including 505.459 death reported to WHO (Din and Boppana, 2020). Since that, a total of 215 countries have been affected by the virus worldwide. The generalized dissemination and infectivity rate of (2019-nCoV) makes it a major pathogen right now. Furthermore, the present review concentrate on the most contemporary clinical information regarding transmission, pathogenesis, clinical manifestation and laboratory diagnosis to effectively manage, prevent, and advise patients worldwide.
History:
Coronaviruses (CoV) belong to major belonging of enveloped single-stranded RNA viruses their diameter ranging from (60-140 nm) while the genomes ranging from 25 to 32 kb, it possesses a spike projections on its outer superficial layer since it appears like a crown under the electron microscope; that is why scientists denominate a coronavirus (Li et al., 2010). Virions are toughly globular and their huge spike (S) glycoprotein that expand (16-21) nm from the envelope of virus (Fig. 1). The family includes two subfamilies, the Coronavirinae and the Torovirinae. The toroviruses are responsible for the enteric form of illness in cattle as well as in humans. The Coronaviridae family, along with the Arteviridae and Roniviridae families, belong to the Nidovirales order. The Arteviridae family includes which is defined as the pathogenic virus of invertebrate. More than 60 coronaviruses (CoVs) were isolated from bats (BtCoV), the majority of which are in the genus beta-coronavirus. Bats act as large (and highly mobile) CoV reservoirs; many species of bats have their own distinctive β CoV, which implies a very long history of development.
Previously four coronaviruses namely HKU1, NL63, 229E, and OC43 have been detected in humans’ circulation, which give rise to minor enteric and respiratory symptoms ranging from cold or flu to much more serious diseases. Its zoonotic disease can infect birds and mammals, including humans (Li et al., 2010; Terada et al., 2014). CoVs were regarded as mere minor human pathogens until 2002 where an outbreak of severe acute respiratory syndrome (SARS), which occurred in 2002, was correlated with a new CoV (SARS CoV) infection, then the sporadic infection became involved in CoV replication, distribution, development, transmission, and pathogenesis. Another (different from SARS-CoV) coronavirus was isolated in 2014 in direct link with an outbreak of the severe respiratory disease in the Middle East, later they named the Middle East respiratory syndrome coronavirus (MERS-CoV), so right now, there were 6 species of corona (other than new SARS-CoV-2) discovered, persist causing sporadic cases of massive respiratory illness (Su et al., 2016; Zaki, 2012).
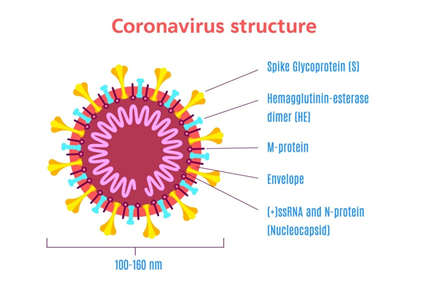
Figure 1. Schematic representation of a coronavirus virion structure (subfamily Coronavirinae).
Foci of the spread of COVID19 pandemics:
The infection began when adults presenting serious pneumonia of unknown cause to local hospitals In December 2019, in Wuhan, the capital of Hubei district, China. Most of those original cases had a regular relation to the wholesale Huanan seafood industry, which also sold live animals. Then, the health authorities and government respond quickly and the monitoring system was triggered, respiratory samples of patients were sent to reference laboratories for etiologic fulfillment. China declared the outbreak to the World Health Organization and on 1st January they closed the Huanan seafood market. The virus was then characterized as coronavirus, which had >95% similarity to the beta (β) genera found in bat coronavirus and >70% similarity to SARS CoV. Screening of samples (environmental samples) from the Huanan seafood market also screened positive (samples containing SARS-CoV-2), environmental samples (585 samples) from the seafood market in Huanan also screened positive (samples containing SARS-CoV-2), indicating that the virus emerged from there (Bai et al., 2020). Then, researchers started to isolate SARS-CoV-2 from the biological samples (lung fluid, blood, and throat swab samples) and revealed that the virus-specific nucleic acid sequences quite vary from the former human coronavirus species. The number of patients increased exponentially, as some of which had not recently visited the live animal market, proposing the actuality that human-to-human dissemination occurred (Yang et al., 2020). This disproved the theory correlating with former COVs, which indicates that virus transmission occurs from animal to human only.
After less than one month, the first fatal case was documented; the enormous transmigration of Chinese through the Chinese New Year sparked the epidemic. For virus sequencing samples from broncho-alveolar lavage fluid isolated for culture, the finding revealed that SARS-CoV-2 was completely variable from SARS-CoV (with about 79% sequence identity) and MERS-CoV (with about 50% sequence identity) than from two bat-derived SARS-like coronaviruses - bat-SL-CoVZC45 (with 87.9% sequence identity) and bat-SL-CoVZXC21 (with 87.2% sequence identity) (Zhao et al., 2020). Many studies also indicated that COVID-19 S-protein, in spite of the variance of its sequence to that of SARS-CoV (Marra et al., 2003), endorsed strong interaction with human ACE2 molecules. A brief study for clarifications is needed, to determine the presence of intermediate hosts that initiated the transmission of the virus to humans (Zhao et al., 2020). The reported hypothesis that the bat may be directly responsible for the transmission of the virus to human is a hypothesis with some confusion for several reasons :(1) The Huanan Seafood Wholesale Market had numerous non-aquatic species (including mammals) available for purchase but no bats were sold; (2) SARS-CoV-2 and their family members, bat-SL-CoVZC45 and bat-SL-CoVZXC21, have a comparatively long branch (sequence identity of less than 90 percent), proposing that such viruses are not the closest relatives of SARS-CoV-2; and (3) in other coronaviruses where bat is an important reservoir such as SARS-CoV and MERS-CoV, other animals have acted as intermediate host (civets and possibly camels, respectively). However, bats do not always need an intermediate host to pass viruses on to humans. In Bangladesh, for example, the Nipah virus is disseminated via bats shedding into raw date palm sap (Wu and McGoogan, 2020).
Pathogenesis:
Even though much is identified about the mortality of the clinical disease, much less is understood about the pathophysiology of the virus. In addition, since specifics of the inflammatory mechanisms to the virus are unclear, likely track of events can be hypothesized based on previous SARS-CoV studies. A cell biology viewpoint is helpful in wording research questions and illustrating the clinical path by concentrating on the aspects of the respiratory tract. According to infected cells, COVID-19 can be categorized into three different phases that lead to different clinical manifestations (Wan et al., 2020).
Stage 1: Asymptomatic stage:
This stage occurs one to two days when virus SARS-CoV-2 inhaled, which tend to attach to epithelial cells in the nasal cavity and initiate replicating through the ACE2 receptor (the main receptor for both SARS-CoV2 and SARS-CoV) (Hoffmann et al., 2020; Sims et al., 2005). In vitro data clarify that the SARS-CoV targeted ciliated cells (primary cells infected in the conducting airways) (Reyfman et al., 2019). This hypothesis may require some clarification because single-cell RNA indicates low levels of ACE2 expression in the conduction of airway cells and no evidence predilection for the cell type (Tang et al., 2005). There is local diffusion of the virus and a restricted innate immune response. At this phase the virus can be revealed by nasal swabs although the viral load may be depressed, this may justify the negativity of results at this stage. Unfortunately, these individuals are infectious at this stage.
Stage 2: Upper airway stage:
In the next few days, the virus proliferates and migrates down the respiratory tract along the conducting airways, which alert more intensive innate immune reaction. Virus (SARS-CoV-2) should be discharged in nasal swabs or sputum secretions. At such time, the disease COVID-19 becomes obvious clinically apparent. The level of CXCL10 (CXCL10 is an interferon responsive gene that has an excellent signal to annoyed ratio in the alveolar type II cell response to both SARS-CoV and influenza) (Qian et al., 2013; Wang et al., 2011; Mason, 2020) Evaluating the innate immune response of the host may enhance forecasts of the disease's later course and may lead to rapid monitoring. The disease will be moderate for about 80 percent of the infected patients and predominantly confined to the upper and conductive airways and by ending this stage, the disease can develop into the third stage (Pneumonia) (Wan et al., 2020). These patients with conservative symptomatic therapy may be monitored at home.
Stage 3: Hypoxia, ground-glass infiltrates:
Worse still, about 20% of the infected patients will progress to stage 3 disease and will develop pulmonary infiltrates and some of these will develop very severe disease. Initial estimates of the fatality rate are around 2%, but this varies markedly with age (Wan et al., 2020). This advancement is linked to the maximum production of pro and anti-inflammatory cytokines including IL2, IL7, IL10, GCSF, and TNFα.
The virus currently hits the lung gas exchange systems and penetrates type II alveolar cells (the type I precursor cells). SARS-CoV replicates and is divided rapidly within type II cells, generates a significant number of viral particles, and the cells induce apoptosis and perish (Wang et al., 2011). The outcome is possibly a self-replicating pulmonary toxin, as the viral particles generated infect cells of type II in adjacent units. A researcher thinks that infected space of the lung will possibly lose most of its type II cells, and an alternative pathway for epithelial restoration will be excited (Mason, 2020; Gu and Korteweg, 2007). Hence, the pathological outcome of SARS and COVID-19 is a widespread alveolar injury with fibrin-rich hyaline membranes and a scarce of multinucleated giant cells (Xu et al., 2020; Ho et al., 2001). Intensive scarring and fibrosis could progress to abnormal lung tissue repair. As an aggressive innate and acquired immune response and epithelial regeneration will be required for rehabilitation, the elderly infected patients are at risk because of their depleted immune response and this may permit the virus to disseminate to the gas exchange units of the lung more readily (Sims et al., 2005; Cheung et al., 2005). There is still limited information and data about the pathogenicity of COVID 19, and all data stated by the authors on the assumption that viral entry is based on SARS-CoV as it looks the same. Unfortunately, the available information about SARS-COV 2 looks like the tip of the iceberg, surely, all inquiries and ambiguities will become clear in the upcoming days or even months and detailed studies on infection and the innate immune response of differentiated primary human lung cells (type II cells) facilitating viral entry will be cut off point.
Table 1: An epidemiological features of SARS CoV, SARS CoV, and MARS CoV
|
|
Year |
Animal reservoir |
Intermediate host |
Receptor |
Incubation period (mean) |
Fatality rate |
R0 |
|
SARS-CoV2 |
2019 |
Bats |
Unknown |
Angiotensin-converting enzyme 2 (ACE2) |
2-14 (5-7) days |
2.3% |
2-2.5 |
|
MARS-CoV |
2012 |
Bats |
Camels |
Dipeptidyl peptidase 4 (DPP4) |
2-13 (5-7) days |
34.4% |
0.7 |
|
SARS-CoV |
2002 |
Bats |
Palm civets |
Angiotensin-converting enzyme 2 (ACE2) |
2-14 (5) days |
9.5% |
1.7-1.9 |
*SARS-CoV-2, severe acute respiratory syndrome coronavirus 2;
*SARS-CoV, severe acute respiratory syndrome coronavirus;
*MERS-CoV, Middle East respiratory syndrome coronavirus;
*R0, reproduction number
Mode of Transmission:
Numerous domestic and wild animals act as coronavirus hosts (reservoir host), including camels, cattle, cats, and bats (Liu et al., 2005). It is well known that animal coronaviruses do not spread among humans (Riou and Althaus, 2020), although, the exclusion occurs in (SARS 2003) and (MERS 2012), which are transmitted by coughing or sneezing predominantly by close contact with infected people by respiratory droplets. Regarding COVID-19 there is three main transmission route described based on the latest guidelines from Chinese health authorities (Li et al., 2020; Nishiura et al., 2020): 1) droplets transmission, 2) contact transmission, and 3) aerosol transmission. Transmission through droplets has been revealed when people in close proximity swallow or snuff the respiratory droplets (generated if infected individual coughs or sneezes); contact transmission takes place when an individual touches up a virus-contaminated surface and thereafter touches his/her mouth, nose, or eyes; and when respiratory droplets remain suspended in the air, an aerosol transmission can happen, then infection arises when a high dose of aerosols is inhaled into the respiratory airways in a comparatively closed surrounding (Li et al., 2020; Tran et al., 2012).
Also, one study indicated the gastrointestinal tract as a prospected transmission route for COVID-19 infection. As many cases had abdominal discomfort and diarrhea symptoms, researchers' outcomes on four datasets with single-cell transcriptomes of digestive systems revealed that ACE2 was extremely expressed in absorptive enterocytes from ileum and colon; hence, COVID 19 virus can be transmitted through ingestion (Li et al., 2020).
A recent study by Diangeng Li et. al, (2020) conducted on Chinese patients after recovery from COVID-19 confirmed that SARS-CoV-2 can be present in the semen of recovered cases, which may be due to the presence of systemic local inflammation. Even if the virus cannot replicate in the male reproductive system, it may persist, probably due to the advantaged immunity of the testes. So, the mode of the sexual transmission of SARS-CoV-2 is not fully understood and needs further studies.
Figure 2: Novel coronavirus SARS-CoV-2, a particle of a transmission electron micrograph isolated from an infected COVID 19 patient.
Clinical manifestation and diagnosis:
Coronaviruses are zoonotic in nature and infect all ages causing symptoms ranging from mild common cold to massive respiratory, enteric, hepatic, and renal manifestation (Tay et al., 2020; Hassan et al., 2020).
The comprehensive clinical picture of SARS COV 2 is still not apparent since the symptoms confirmed varied from the mild treated symptoms to extreme fatal symptoms (Huang et al., 2020). Generally and commonly reported symptoms are fever (≥ 38°C, 100.4°F), cough, myalgia or fatigue, pneumonia, and complicated dyspnea, whereas less common reported symptoms include headache, diarrhea, hemoptysis, runny nose, and phlegm producing cough (Huang et al., 2020). Generally, patients with minor symptoms have been observed to recover after 1 week although serious cases have experienced progressive respiratory failure due to alveolar destruction from the virus, which can end in death. Middle-aged and elderly patients with pre-existing diseases (tumor surgery, cirrhosis, hypertension, coronary heart disease, diabetes, and Parkinson’s disease) are at risk for severe COVID 19 as their immune status is diminished and reduced (Adhikari et al., 2020).
Laboratory and radiology diagnosis:
A sophisticated criterion has been confirmed by the U.S. CDC for persons under investigation (PUI) (person with fever (≥ 38°C, 100.4°F), and pneumonia or acute respiratory distress syndrome (based on the clinical or radiological evidence), history of travel to areas of the persistent local transmission 14 days ago or contact with patients with similar travel history); here, an instant prevention and infection control measures are warranted. For better isolation of the virus, WHO suggests that samples should be taken from both the upper and lower respiratory tract. This can be accomplished via expectorated sputum, bronchoalveolar lavage, or endotracheal aspirate, also virus may be isolated from the stool and blood in severe cases. Then, these samples are evaluated for viral RNA by real-time polymerase chain reaction (RT-PCR). When a positive finding is detected, the repetition of the test for reverification is necessary. Repeat tests also are required when the results are negative in symptomatic patients. Generally, there are other non-specific laboratory tests that should be done. The white blood cell (WBC) count is often normal or low. Lymphopenia (lymphocyte count <1000) is critical, which is correlated with deteriorated cases. The platelet count is often normal or mildly low, while C Reactive Protein (CRP) and Erythroid Sedimentation Rate (ESR) are generally elevated but procalcitonin levels are usually normal. A high procalcitonin level may indicate a bacterial co-infection. The ALT/AST, prothrombin time, creatinine, D-dimer, CPK, and LDH may be elevated and high levels are related to the massive form of the disease (Chen et al., 2020).
Regarding radiology finding, the X-ray in the chest (CXR) normally reveals bilateral infiltrates, although it can be normal in early illness. The CT is more sensitive and specific (as it is abnormal even in asymptomatic patients), generally infiltrates appear as ground-glass opacities and subsegmental consolidation. Actually, unusual CT scans were used to diagnose COVID-19 with negative molecular diagnosis in suspicious cases; most of these patients had positive molecular tests on repeat tests (Huang et al., 2020).
Treatment:
Until now, there is no approved treatment for COVID19 and the candidate vaccine is under development; the protocol followed for the treatment of infected patients is based on the experience with SARS and MERS. Treatment is essentially supportive and symptomatic. Moderate infection should be managed at home by notifying about danger signs. The standard guidelines are the management of hydration and nutrition, as well as a regular checkup of fever and cough. In confirmed cases, the routine use of antibiotics and antivirals like oseltamivir should be averted except when co-infections are suspected or verified. Hypoxic patients may require mechanical oxygen ventilation; also renal replacement therapy is indicated in some cases. Corticosteroids are contraindicated and unproven; while current international consensus, WHO and Chinese protocol support the use of short-term therapy with low-to-moderate dose corticosteroids in COVID-19 ARDS (Russell et al., 2020; Zhao et al., 2020; Hassan et al., 2020). Another suggested medicines for therapy are an antiviral drug (arbidol), intravenous immunoglobulin, interferons, plasma of patients recovered from COVID-19, as well as chloroquine, although there is controversy over its use (Bassetti et al., 2020; Yu et al., 2020; Liu et al., 2005; Chan et al., 2020). Additionally, alternative medicine recommendations about using traditional herbs are critical and may play an important role in increasing the cure rate (Bassetti et al., 2020), but we need more evidence before these drugs are recommended.
Prevention and control:
As there is no confirmed treatment for SARS COV 2, the preventive measures are critical and must concentrate on improving protocols for infection control, self-isolation, and patient isolation during clinical care. Although prevention and control are difficult right now, because of ambiguity surrounding the virus and the lack of quite knowledge concerning its spread (Jie et al., 2020).
Individuals must be asked at the community level to avoid congested places and wear masks in public, especially in crowded places. As an alternative measure, cough hygiene should be practiced also hand hygiene such as (repeatedly wash every 15-20 min and using hand sanitizers) must be obligatory for all populations. Surgical masks should be applied for patients with respiratory problems (Li et al., 2020; Guo et al., 2020). Immunocompromised people are recommended to avoid public congestions. The WHO has guidance toward direct contact with infected patients, domestic animals, as well as wildlife (Holshue et al., 2020; Singhai, 2020; Chang et al., 2020). Departments of emergency medicine should enforce strict hygienic measures to control infections. Healthcare personnel must use personal protective equipment such as N95 masks, FFP3 masks, eye protection, gloves, and gowns as they have the highest risk for infection with COVID-19, reports in the SARS outbreak of 2002, about 21% of those affected were healthcare workers (Chang et al., 2020; Ahn et al., 2019; Wang et al., 2020).
Finally, COVID 19 is a real catastrophe, we should deal with it with great care it is a highly transmissible disease, which has been put all world into a crisis not only medical but also major economic crisis, due to outbreak and pandemic of the SARS COV 2 virus.
Prospective:
Extensive research efforts on vaccine development is critical especially in the term of molecular immunology and immunogenicity of the emerged virus. The potential role of availing T cell and B cell responses for coronavirus vaccination should also be deemed. Those resistant have been shown to be permanent and protective in animal models. Also, the possible role of pro and anti-inflammatory cytokines must be regarded.
Conclusions
The COVID-19 pandemic is an emerging disease that disseminated all over the world at a horrible rate dramatically. It has triggered more infections and deaths than SARS or MERS due to its high speed of transmission so SARS-CoV-2 is more infectious discovered coronavirus, and the exact pathogenicity of the virus is not clear yet. The elderly, as well as immunocompromised patients present the highest risk of death. The rapid dissemination of the disease requires rigorous protocols of monitoring and rapid intervention assist isolation of the virus, and serve the life of patients and community by avoiding further transmission as no approved medication and vaccine is under development. The present treatment protocols are just for symptomatic care and oxygen therapy. Prophylactic vaccination is crucial for the future prevention of COV-related epidemic or pandemic.
Acknowledgment:
This publication was supported by the Deanship of scientific research at Prince Sattam bin Abdul-Aziz University.
Conflict of interest:
The author declares that she has no competing interests.
Research funding:
None declared.
References
Adhikari, S. P., Meng, S., Wu, Y. J., Mao, Y. P., Ye, R. X., Wang, Q. Z., ... & Zhou, H. (2020). Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infectious diseases of poverty, 9(1), 1-12.
Ahn, D. G., Shin, H. J., Kim, M. H., Lee, S., Kim, M. H. S., Myoung, J., ... & Kim, S. J. (2019). Current Status of Epidemiology. Diagnosis, Therapeutics, and Vaccines for Novel Coronavirus Disease, 2020.
Alshammari, E. (2020). Implementing eOSCE During COVID-19 Lockdown. Journal of Advanced Pharmacy Education & Research| Jan-Mar, 10(1), 175.
Bai, Y., Yao, L., Wei, T., Tian, F., Jin, D. Y., Chen, L., & Wang, M. (2020). Presumed asymptomatic carrier transmission of COVID-19. Jama, 323(14), 1406-1407.
Bassetti, M., Vena, A., & Giacobbe, D. R. (2020). The novel Chinese coronavirus (2019‐nCoV) infections: Challenges for fighting the storm. European journal of clinical investigation, 50(3), e13209.
Chan, K. W., Wong, V. T., & Tang, S. C. W. (2020). COVID-19: An update on the epidemiological, clinical, preventive and therapeutic evidence and guidelines of integrative Chinese–Western medicine for the management of 2019 novel coronavirus disease. The American journal of Chinese medicine, 48(03), 737-762.
Chang, D., Xu, H., Rebaza, A., Sharma, L., & Cruz, C. S. D. (2020). Protecting health-care workers from subclinical coronavirus infection. The Lancet Respiratory Medicine, 8(3), e13.
Chen, N., Zhou, M., Dong, X., Qu, J., Gong, F., Han, Y., ... & Yu, T. (2020). Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. The Lancet, 395(10223), 507-513.
Cheung, C. Y., Poon, L. L., Ng, I. H., Luk, W., Sia, S. F., Wu, M. H., ... & Peiris, J. S. (2005). Cytokine responses in severe acute respiratory syndrome coronavirus-infected macrophages in vitro: possible relevance to pathogenesis. Journal of virology, 79(12), 7819-7826.
Din, M. A. U., & Boppana, L. K. T. (2020). An update on the 2019-nCoV outbreak. American Journal of Infection Control, 48(6), 713. 10.1016/j.ajic.2020.01.023
Gu, J., & Korteweg, C. (2007). Pathology and pathogenesis of severe acute respiratory syndrome. The American journal of pathology, 170(4), 1136-1147.
Guo, Y. R., Cao, Q. D., Hong, Z. S., Tan, Y. Y., Chen, S. D., Jin, H. J., ... & Yan, Y. (2020). The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak–an update on the status. Military Medical Research, 7(1), 1-10.
Hassan, S. A., Sheikh, F. N., Jamal, S., Ezeh, J. K., & Akhtar, A. (2020). Coronavirus (COVID-19): a review of clinical features, diagnosis, and treatment. Cureus, 12(3).
Ho, J. C., Chan, K. N., Hu, W. H., Lam, W. K., Zheng, L., Tipoe, G. L., ... & Tsang, K. W. (2001). The effect of aging on nasal mucociliary clearance, beat frequency, and ultrastructure of respiratory cilia. American journal of respiratory and critical care medicine, 163(4), 983-988.
Hoffmann, M., Kleine-Weber, H., Schroeder, S., Krüger, N., Herrler, T., Erichsen, S., ... & Müller, M. A. (2020). SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell.
Holshue, M. L., DeBolt, C., Lindquist, S., Lofy, K. H., Wiesman, J., Bruce, H., ... & Diaz, G. (2020). First case of 2019 novel coronavirus in the United States. New England Journal of Medicine.
Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., ... & Cheng, Z. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The lancet, 395(10223), 497-506.
Huang, P., Liu, T., Huang, L., Liu, H., Lei, M., Xu, W., ... & Liu, B. (2020). Use of chest CT in combination with negative RT-PCR assay for the 2019 novel coronavirus but high clinical suspicion. Radiology, 295(1), 22-23.
Jie, Z., He, H., Xi, H., & Zhi, Z. (2020). Multicenter Collaboration Group of Department of Science and Technology of Guangdong Province and Health Commission of Guangdong Province for Chloroquine in the Treatment of Novel Coronavirus Pneumonia. Expert Consensus on Chloroquine Phosphate for the Treatment of Novel Coronavirus Pneumonia [in Chinese], 10, 1001-0939.
Lestari, K., Sitorus, T., Instiaty, S. M., & Levita, J. (2020). Molecular Docking of Quinine, Chloroquine and Hydroxychloroquine to Angiotensin Converting Enzyme 2 (ACE2) Receptor for Discovering New Potential COVID-19 Antidote. Journal of Advanced Pharmacy Education & Research| Apr–Jun, 10(2).
Li, D., Jin, M., Bao, P., Zhao, W., & Zhang, S. (2020). Clinical characteristics and results of semen tests among men with coronavirus disease 2019. JAMA network open, 3(5), e208292-e208292.
Li, J., Li, J. J., Xie, X., Cai, X., Huang, J., Tian, X., & Zhu, H. (2020). Game consumption and the 2019 novel coronavirus. The Lancet Infectious Diseases, 20(3), 275-276.
Li, Q., Guan, X., Wu, P., Wang, X., Zhou, L., Tong, Y., ... & Xing, X. (2020). Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. New England Journal of Medicine.
Liu, S., Chen, J., Chen, J., Kong, X., Shao, Y., Han, Z., ... & Liu, M. (2005). Isolation of avian infectious bronchitis coronavirus from domestic peafowl (Pavo cristatus) and teal (Anas). Journal of General Virology, 86(3), 719-725.
Liu, Y. C., Huang, V., Chao, T. C., Hsiao, C. D., Lin, A., Chang, M. F., & Chow, L. P. (2005). Screening of drugs by FRET analysis identifies inhibitors of SARS-CoV 3CL protease. Biochemical and biophysical research communications, 333(1), 194-199.
Marra, M. A., Jones, S. J. M., Astell, C. R., Holt, R. A., & Brooks‐Wilson, A. B. YSN 2003. The genome sequence of the SARS‐associated coronavirus. Science, 300(5624), 1399-1404.
Mason, R. J. (2020). Pathogenesis of COVID-19 from a cell biology perspective.
Meconcelli, G., Bazzoni, G., & Casu, C. (2020). Auriculotherapy for Stress Management as Self-Help in Isolation Situations (COVID 19). International Journal of Pharmaceutical and Phytopharmacological Research, 10(3), 1-2.
Mohammadzadehgodini, M. (2020). Coronavirus treatment with colostrum. Archives of Pharmacy Practice, 11(1):76-80.
Nishiura, H., Jung, S. M., Linton, N. M., Kinoshita, R., Yang, Y., Hayashi, K., ... & Akhmetzhanov, A. R. (2020). The extent of transmission of novel coronavirus in Wuhan, China, 2020.
Qian, Z., Travanty, E. A., Oko, L., Edeen, K., Berglund, A., Wang, J., ... & Mason, R. J. (2013). Innate immune response of human alveolar type ii cells infected with severe acute respiratory syndrome–coronavirus. American journal of respiratory cell and molecular biology, 48(6), 742-748.
Reyfman, P. A., Walter, J. M., Joshi, N., Anekalla, K. R., McQuattie-Pimentel, A. C., Chiu, S., ... & Verma, R. (2019). Single-cell transcriptomic analysis of human lung provides insights into the pathobiology of pulmonary fibrosis. American journal of respiratory and critical care medicine, 199(12), 1517-1536.
Riou, J., & Althaus, C. L. (2020). Pattern of early human-to-human transmission of Wuhan 2019 novel coronavirus (2019-nCoV), December 2019 to January 2020. Eurosurveillance, 25(4), 2000058.
Russell, C. D., Millar, J. E., & Baillie, J. K. (2020). Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. The Lancet, 395(10223), 473-475.
Sims, A. C., Baric, R. S., Yount, B., Burkett, S. E., Collins, P. L., & Pickles, R. J. (2005). Severe acute respiratory syndrome coronavirus infection of human ciliated airway epithelia: role of ciliated cells in viral spread in the conducting airways of the lungs. Journal of virology, 79(24), 15511-15524.
Singhai, T. (2020). A review of the coronavirus disease-2019. Indian J Pediatr, 87, 281-286.
Su, S., Wong, G., Shi, W., Liu, J., Lai, A. C., Zhou, J., ... & Gao, G. F. (2016). Epidemiology, genetic recombination, and pathogenesis of coronaviruses. Trends in microbiology, 24(6), 490-502.
Tang, N. L. S., Chan, P. K. S., Wong, C. K., To, K. F., Wu, A. K. L., Sung, Y. M., ... & Lam, C. W. K. (2005). Early enhanced expression of interferon-inducible protein-10 (CXCL-10) and other chemokines predicts adverse outcome in severe acute respiratory syndrome. Clinical chemistry, 51(12), 2333-2340.
Tay, M. Z., Poh, C. M., Rénia, L., MacAry, P. A., & Ng, L. F. (2020). The trinity of COVID-19: immunity, inflammation and intervention. Nature Reviews Immunology, 1-12.
Terada, Y., Matsui, N., Noguchi, K., Kuwata, R., Shimoda, H., Soma, T., ... & Maeda, K. (2014). Emergence of pathogenic coronaviruses in cats by homologous recombination between feline and canine coronaviruses. PLoS One, 9(9), e106534.
Tran, K., Cimon, K., Severn, M., Pessoa-Silva, C. L., & Conly, J. (2012). Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PloS one, 7(4), e35797.
Wan, Y., Graham, R., Baric, R. S., & Li, F. (2020). An analysis based on decade-long structural studies of SARS 3, JVI Accepted Manuscript Posted Online 29 January 2020. J. Virol.
Wang, J., Nikrad, M. P., Phang, T., Gao, B., Alford, T., Ito, Y., ... & Mason, R. J. (2011). Innate immune response to influenza A virus in differentiated human alveolar type II cells. American journal of respiratory cell and molecular biology, 45(3), 582-591.
Wang, Y., Wang, Y., Chen, Y., & Qin, Q. (2020). Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID‐19) implicate special control measures. Journal of medical virology, 92(6), 568-576.
Wu, Z., & McGoogan, J. M. (2020). Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. Jama, 323(13), 1239-1242.
Xu, Z., Shi, L., Wang, Y., Zhang, J., Huang, L., Zhang, C., ... & Tai, Y. (2020). Pathological findings of COVID-19 associated with acute respiratory distress syndrome. The Lancet respiratory medicine, 8(4), 420-422.
Yang, X., Yu, Y., Xu, J., Shu, H., Liu, H., Wu, Y., ... & Wang, Y. (2020). Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. The Lancet Respiratory Medicine.
Yu, F., Du, L., Ojcius, D. M., Pan, C., & Jiang, S. (2020). Measures for diagnosing and treating infections by a novel coronavirus responsible for a pneumonia outbreak originating in Wuhan, China. Microbes and infection.
Zaki, A. M. (2012). van BS, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. N Engl J Med, 367(19), 1814-20.
Zhao, J. P., Hu, Y., Du, R. H., Chen, Z. S., Jin, Y., Zhou, M., ... & Cao, B. (2020). Expert consensus on the use of corticosteroid in patients with 2019-nCoV pneumonia. Zhonghua jie he he hu xi za zhi= Zhonghua jiehe he huxi zazhi= Chinese journal of tuberculosis and respiratory diseases, 43(3), 183-184.
Zhao, Y., Zhao, Z., Wang, Y., Zhou, Y., Ma, Y., & Zuo, W. (2020). Single-cell RNA expression profiling of ACE2, the putative receptor of Wuhan 2019-nCov. BioRxiv.








