The Effect of Dual-Task Training on Dynamic Postural Control in the Subjects with Functional Ankle Instability
Atefeh Onegh, Asghar Akbari*, Fateme Ghiasi, Mohammad Hosseinifar, Ahmadreza Asgari Ashtiani
Abstract
Background and Objective: Recurrent ankle sprains usually happen when a person does two or more tasks simultaneously. This study was aimed to investigate the effect of dual-task training (DTT) on dynamic postural control (DPC) in individuals with functional ankle instability (FAI). Method: This single-blind randomized controlled trial was conducted in Zahedan University of Medical Sciences in 2015. Thirty-two individuals with FAI were selected using a convenience sampling method and randomly assigned into two groups of Biodex balance training and DTT. Each group received its intervention for 4 weeks, three days a week, for 30 minutes per day. Overall stability index, anterior-posterior, and medial-lateral indices were measured by Biodex balance system in single and double-leg stances with open and closed eyes, before and after the intervention. Paired samples and independent t-tests were used for data analysis. Results: The results showed that overall stability, anterior-posterior, and medial-lateral stability indices improved significantly after performing DTT in all cases (P<0.05). In the balance training group, the medial-lateral stability index in a double-leg stance with open eyes at easy stability level and in double-leg stance with closed eyes at difficult stability level were significantly changed (P <0.05). However, in other cases, there were no significant changes (P<0.05). There were no differences between the two groups regarding the study variables (P<0.05). Conclusion: Dual-task training improved more balance indices compared to Biodex balance training. Hence, it is recommended that DTT be included in a physiotherapy program for people with FAI.
Key words: Functional Ankle Instability, Balance Training, Biodex, Dual-Task Training, Dynamic Postural Control
Abstract
Background and Objective: Recurrent ankle sprains usually happen when a person does two or more tasks simultaneously. This study was aimed to investigate the effect of dual-task training (DTT) on dynamic postural control (DPC) in individuals with functional ankle instability (FAI). Method: This single-blind randomized controlled trial was conducted in Zahedan University of Medical Sciences in 2015. Thirty-two individuals with FAI were selected using a convenience sampling method and randomly assigned into two groups of Biodex balance training and DTT. Each group received its intervention for 4 weeks, three days a week, for 30 minutes per day. Overall stability index, anterior-posterior, and medial-lateral indices were measured by Biodex balance system in single and double-leg stances with open and closed eyes, before and after the intervention. Paired samples and independent t-tests were used for data analysis. Results: The results showed that overall stability, anterior-posterior, and medial-lateral stability indices improved significantly after performing DTT in all cases (P<0.05). In the balance training group, the medial-lateral stability index in a double-leg stance with open eyes at easy stability level and in double-leg stance with closed eyes at difficult stability level were significantly changed (P <0.05). However, in other cases, there were no significant changes (P<0.05). There were no differences between the two groups regarding the study variables (P<0.05). Conclusion: Dual-task training improved more balance indices compared to Biodex balance training. Hence, it is recommended that DTT be included in a physiotherapy program for people with FAI.
Key words: Functional Ankle Instability, Balance Training, Biodex, Dual-Task Training, Dynamic Postural Control
Introduction
An ankle sprain is one of the prevalent injuries among athletes and the public. (Webster and Gribble, 2013) Generally, it accounts for 25% of all sports injuries. (Rotem-Lehrer and Laufer, 2007) There are no precise statistics on ankle sprains in Iran; but, it has been reported at the range of 23,000-27,000 a day in the United States and 30,000,000 in England per year. This is while 55% of people have not referred to medical centers for treatment. Hence, the true value of the prevalence of this injury cannot be estimated. (Wikstrom et al., 2005). 80% of people experience repeated ankle sprains during daily activities. (Webster and Gribble, 2013; Akhbari et al., 2007; Gribble and Robinson, 2009)
A recurring ankle sprain can cause FAI, (Lehman, 2006) and this functional instability can eventually end in osteoarthritis in the ankle. (Willems et al., 2005) FAI is a kind of disability reported by the patient as a giving way. A significant feature of this type of instability is that the patient complains of a feeling of giving way, without increased ankle range of motion or specific clinical symptoms. (Freeman et al., 1965)
Studies have shown that individuals with chronic ankle instability have problems in postural control. (Hubbard and Kaminski, 2002; Ross et al., 2005; Rose et al., 2000; Docherty et al., 2006) In a study on FAI patients, it was found that although these patients complained of ankle giving way, this injury had no real negative effects on ankle function. Some researchers argue that these people face problems and reduction in performance levels when they want to do activities like walking, running and jumping, and the like alongside another task, such as moving a ball on the field while running. Hence, evaluating the skills of these people by integrating them with a secondary motor or cognitive task can be helpful in identification of the mechanisms and reaching new therapeutic approaches. (Demeritt et al., 2002)
Scholars have examined the dependence of motor control on attention to study the effect of the cognitive system on motor control. Attention can be defined as the capacity to process information consciously. (Woollacott and Shumway-Cook, 2002) There is a hypothesis on processing capacity that believes that processing capacity of each individual is limited and that a certain amount of capacity is needed to perform each task. (Woollacott and Shumway-Cook, 2002) Thus, when two tasks are done simultaneously and the attention needed by these two tasks exceeds the overall capacity, performing one or both of them decreases to some extent, which is called interference. (Woollacott and Shumway-Cook, 2002; Shumway-Cook and Woollacott, 2000) One of the methods used in the studies to examine attention needs is dual-task assignment. (Huang and Mercer, 2001) The competition between postural control and another secondary task over attention resources can cause changes in postural control parameters. (Dault et al., 2001; Pellecchia, 2003) According to various studies, this competition is more manifested in elderly and neurological and vestibular patients. (O'Shea et al., 2002; Huxhold et al., 2006) The studies have shown that an increase in the difficulty of cognitive assignment while performing a balance task can lead to an increase in postural sway (Pellecchia, 2003; Melzer et al., 2001), a decrease in postural sway, (Dault et al., 2001; Andersson et al., 2002) or no change. (Teasdale et al., 1993)
Even though numerous studies have examined the postural reactions due to the external postural perturbations in musculoskeletal disorders, (Vanicek et al., 2009; Ferber et al., 2003; Johansson et al., 1991; Ihara et al., 2008; Lysholm et al., 1998) few studies have examined the effect of motor planning on the balance reactions in individuals with musculoskeletal injuries. (Geurts and Mulder, 1994) Given the need for postural control for a percentage of attention resources and the central processing system disorder in musculoskeletal patients, one of the problems in these patients is assigning attention to postural control. Thus, assuming that cognitive exercise along with balance training can improve postural control in individuals with musculoskeletal disorders including FAI, and as the common therapeutic strategies used by therapists to prevent recurrence of ankle sprains are not suitable and the therapeutic efforts should emphasize reducing the risk of ankle sprain. (Beckman and Buchanan, 1995; Hertel, 2002) The purpose of the study was to examine the effect of DTT on DPC in people with FAI.
Method
Study design: The study was a single-blind randomized controlled trial. Thirty-two individuals with FAI were randomly assigned into two groups of Biodex balance training (n= 15) and DTT (n= 17). The patients were unaware of the study theory and they had been informed that “The study tries to determine the difference between the effect of Biodex balance training and DTT, both of which improve postural stability.” The participants in both groups were treated for 4 weeks, three sessions a week and each session for 30 minutes. (Akhbari et al., 2007) Study variables were measured and recorded before and after the intervention.
Study population and the patients’ screening: 32 individuals with FAI were selected using a convenience sampling method. Inclusion criteria were unilateral functional ankle instability with at least one sprain in the last year, feeling of frequent giving way, lack of mechanical ankle instability, negative anterior drawer test, talar dislocation, history of vertigo and fainting, ankle joint pain or inflammation, visual, auditory or verbal disorders, musculoskeletal disorders in the spine and lower extremity, and being 18 to 52 years old. The exclusion criteria were the patient's unwillingness to continue the treatment, symptoms during the treatment, receiving another treatment during the study, and the patient's failure to progress in the early stages of attention training. The eligible individuals were enrolled after signing the informed consent form. The study was approved by the Scientific Committee and Ethics Committee of Zahedan University of Medical Sciences. The study is recorded in Iran Clinical Trial Research Center System as IRCT201604251675N13. The rights of the participants were maintained at all times.
Data collection: The individuals were interviewed and examined to ensure they met the inclusion and exclusion criteria. A tape measure with centimeter precision was used to measure the individuals' height. A digital scale was used to measure the individuals' weight (to calculate body mass index (BMI)) and the Biodex balance system was used to measure balance indices.
Randomization: The individuals were assigned to the intended groups as three-person randomized blocks.
Evaluation of dynamic balance indices
Overall stability indices, anterior-posterior and lateral stability indices were measured by the Biodex SD Balance System (Balance System SD 950-304 Model SW45-30D-E6N, Biodex Medical System, Inc., New York, USA).
In this device, a small computer with keys and a screen is mounted upright on a pole, so that the subject is in front of it when standing on the force plate. (Docherty et al., 2006) The force difficulty can be adjusted as well; i.e., the system can vary the degree of difficulty from 1 (least stable) to 12 (most stable). (Docherty et al., 2006)
Postural Stability was used in this test. The ability to maintain stability is known as the stability index. The individual score in this test shows the degree of deviation from the center. Thus, a lower score is more desirable than a higher score.
Before starting the test, a general explanation of the procedure was given to the candidate. The standing manner on the plate was first removing shoes and socks and then standing on the device's plate. They were asked to try to hold the marker on the device's screen in the center of the circle for some seconds. During this stage, the patient could change the location of his leg to have the best stance to maintain the marker in the center of the circle. Then the force plate was fixed and the angle and coordinates of the leg position were recorded on the Biodex force plate. This state was considered as the best condition in which the individual could maintain the stability of the unstable plate and the leg was placed in the recorded state in all tests. (Lajoie et al., 1993; Rowe et al., 1999) To test on one leg, the patient was placed on the affected leg with the eyes open, the opposite leg was behind the ankle, and the hands were crossed on the chest. To test both legs, the individuals stood once with open eyes and then closed eyes on two legs with the hands crossed on the chest. All these states were tested at 8 (easy) and 5 (difficult) stability level. (Rahnama et al., 2010) The individual then held the device' marker at the center of the screen, with no help of hands and only by shifting its center of gravity by the trunk and shifting the weight on the legs. The duration of each test was 20 seconds, the repetition of the tests was 3 times, and the rest time between tests was 10 seconds. (Greve et al., 2007; Vaseghnia et al., 2008; Farahpour et al., 2004)
Prior to the test and before the intervention, the subjects were pre-tested to get familiar with the device and testing method. The postural dynamic stability test was performed in a double-leg stance with open and closed eyes and a single-leg stance (right and left) with open eyes.
Intervention method
Balance training: Those in the balance-training group were trained using a Biodex balance system and the training mode program. The degree of difficulty of Biodex stability level was progressed to level 5 from the static mode each week. (Docherty et al., 2006) The degree of difficulty of Biodex stability level changed from 12 to 10 in the first session, from 12 to 8 in the second, and from 12 to 5 in the third session, which was repeated in the following weeks. During the exercise, the subjects were standing with their hands crossed tied up on their chests to try to hold the marker displayed on the screen of the device in the center of the circle.
DTT: Those in this group performed Biodex balance exercises simultaneously with attention training, which included some hierarchically organized tasks that included various components of attention including continuous, selective, alternating, and divided attention. (Sohlberg and Mateer, 2017) Continuous attention is maintaining a steady behavioral response during repetitive and continuous activities. The study used visual feedback to train the patient. Selective attention is maintaining a behavioral or cognitive response in facing distracting stimuli. In this study, visual and auditory stimuli were used for training. Alternating attention measures the capacity for mental flexibility. In this study, the patients were asked to memorize a random number on the monitor and then subtract it or added to the next random number on the screen. Divided attention refers to the ability to respond to two or more tasks simultaneously. In this study, visual and auditory tasks were used for training. All levels of these exercises were performed in Cogniplus software. (Sohlberg and Mateer, 2017; Shehab, 2012; Heim et al., 2015; Sturm et al., 2015; Hagovská and Olekszyová, 2016; Schuhfried, 2007) Cogniplus software is a training system for practicing cognitive functions, developed by Professor Walter Strom et al. at Schuhfried Co. This software is a smart interactive system that automatically detects and adjusts the patient's level of ability. This software is designed by computer game programmers similar to everyday life and is applicable to all levels of cognitive ability like head trauma and attention problems. The process of training individuals in this group was similar to the balance training group, except that the subjects performed Biodex balance training simultaneously with attention training. To do the exercise, the individuals stood on the device on two legs with their hands crossed on the chest and the computer placed in front of them for attention exercise. In the first week, continuous attention training, in the second week selective attention, in the third week alternating attention, and in the fourth week, divided attention were added to Biodex balance training.
Determining the sample size: The number of samples was determined according to a pilot study. In doing so, at first 10 patients were selected and randomly divided into two study groups and the main stage of research was performed on them. According to the mean and standard deviation of these two groups, the sample size for the original study was estimated at 95% confidence and 90% test power.
Statistical analysis: Data were analyzed in SPSS 17. Kolmogorov–Smirnov test (K–S test) was used to examine the normality of the data. Levene's test was used to compare variances. A paired-samples t-test was used to compare the quantitative data before and after the intervention. An independent t-test was used to compare the quantitative data between the two groups. For statistical comparisons, the significance level (α) was lower than 5%.
Results
Table 1 presents the demographic information of the participants. K-S test showed that the distribution of all data was normal (P<0.05) (Tables 1-4). The results of the pilot study showed that 15 individuals were required for each group, 42 enrolled at the beginning and 32 completed the study (Figure 1-4).
Mean and standard deviation of the data for overall stability, anterior-posterior and lateral stability indices in a single-leg and double-leg stances in both open and closed eyes and at stability levels of 8 and 5 were compared. Then the pre and post-treatment results of the two groups and the P-value for the comparison of the results after the treatment with the pre-treatment and the comparison of the post-treatment results between the two groups and the P-value for the comparison of the post-treatment results are given in Table 2-4.
Intra-group comparison
Balance training group: The mean overall dynamic stability index was significant in all states (P<0.05). Anterior-posterior stability index showed significant results (P<0.05) except for single leg stance at level 5 (P<0.05). The mean lateral stability index showed significant changes only in double-leg stance with open eyes at stability level 8 and in double-leg stance with closed eyes at stability level 5 (P<0.05). However, in the other states, the mean lateral stability index did not change significantly (P<0.05).
DTT group: Overall, anterior-posterior and lateral stability indices showed significant changes after training (P<0.05) (Table 2).
Inter-group comparisons: We compared the pre-study data between the two groups to test the accuracy of the randomization process. The results showed no differences between the two groups in terms of the variables studied and the patients were matched in the two groups (p>0.05). There were no significant differences between the two groups after the treatment (p>0.05) (Table 2).
Discussion
The results of the study supported a major part of the first hypothesis of the study (reduction in dynamic anterior-posterior instability after balance training) a part of the third hypothesis (reduction in dynamic lateral instability after balance training), and the fifth hypothesis (reduction in overall dynamic instability after balance training). It also supports the second, fourth, and sixth hypotheses of the study stating reduction in dynamic anterior-posterior instability, dynamic medial-lateral instability, and overall dynamic instability after DTT. However, the seventh, eighth, and ninth hypotheses stating more reduction in instability in the DTT group compared to the balance training group were not supported.
The results showed that balance training improves overall stability indices. In this study, dynamic anterior-posterior instability after balance training did not decrease significantly only while standing on one leg at stability level of 5, which could be attributed to a more difficult balance task, as in this case the area under the leg is in the most unstable state and more effort is needed to maintain balance. (Rahnama et al., 2010) Lateral stability index was significant only when standing on two legs with eyes open at level 8 and standing on two legs with eyes closed at level 5. In FAI, lateral stability is affected more due to the damage to lateral ligament injury; (Jain et al., 2016) thus, training that is more specialized is needed to improve lateral instability. Thus, our balance exercises may not have been enough to improve lateral instability on one leg. In a study on people with ankle instability, Youssef et al. (2018) found that exercises on two legs were more effective on the overall and anterior-posterior stability index but did not have a significant effect on the lateral stability index. However, single-leg balance exercises are effective on all stability indices. They concluded that exercises on both legs emphasized lateral stability and less focus. (Youssef et al., 2018) Akbari et al. (2014) showed that the effect of the balance training programs with Biodex balance system on lateral stability indices is less.
The study by Rozzi et al. (1999) supports the results of our study. They trained individuals with FAI on a single leg for four weeks using a Biodex machine and concluded that Biodex balance training is an effective tool to improve the deep sense of the unstable ankle joint. (Rozzi et al., 1999) A slight difference between our results and that of Rozzi may be due to the fact that exercises on two legs were less effective in lateral stability than standing on one leg in our study. Biodex showed little effect on lateral stability because of the 18 stability indices measured in this study. In the balance training group, only 5 indices did not show significant changes after the exercise, 4 of which were related to the lateral stability index.
Elis and Rosenbaum (2001) showed a decrease in postural oscillation in the medial-lateral direction in individuals with ankle instability, which may be due to the nature of the exercise in this study. During the exercises, the individual was standing on one leg, the lower limb was in external rotation, and the knee was bent. This state causes the movement in the inner-outer direction to be mainly controlled by the subtalar joint, whereas the movement in the anterior-posterior direction is controlled by the tibiotalar joint. Thus, the results in this study were mainly due to the focus of practice on the subtalar joint. (Eils and Rosenbaum, 2001)
The findings of Hale et al. (2007) are contradictory to our results. They did not observe a significant change in postural deviation control after a 4-week rehabilitation program by evaluating the center of pressure excursion velocity. (Hale et al., 2007) These inconsistent results may be due to the sensitivity of the measurements and the tools used. The instrument used in the study by Hale et al. was AMTI Accusway force plate interfaced with Swaywin software. Moreover, the parameter measured in the study by Hale et al. was the changes in the displacement velocity of the center of pressure; whereas, in our study the displacement angle of the center of gravity has been estimated. Measuring the pressure-center displacement velocity changes seems to be more sensitive than the center of gravity displacement changes.
In this study, anterior-posterior, and lateral stability indices showed significant improvement after DTT. There are no studies to date to investigate the effect of DTT on balance in individuals with FAI and even other musculoskeletal injuries, but the effect of cognitive task training on balance training in elderly and injured individuals. Neurologic studies have shown that this type of exercise has favorable effects on postural control.
Sinaei et al. (2017) showed that balance training alone and in dual-task cases can improve the level of balance ability and quality of life in the elderly, but there were no significant differences between the two groups due to the lack of participation. The study found participants in the study and lacking long-term follow-up. (Sinaei et al., 2016) Elhinidi et al. (2016) examined the effect of DTT on postural stability of hemiparetic children. 30 patients were included in this study, and randomly divided into two equal groups. Both groups received conventional physiotherapy treatment and the study group performed a cognitive exercise with balance training (DTT). Although both groups showed a significant improvement in overall, anterior-posterior and lateral stability indices compared to pre-training, DTT group showed greater improvement in all stability indices than the control group. They attributed this to the effect of the dual-task program on activating new pathways in the central nervous system for postural control. (Elhinidi et al., 2016) In another study by Konak et al. (2016) on elderly people with osteoporosis, they concluded that both balance and dual-task training had an effect on static and dynamic balance in the elderly, but dual-task training provided greater improvement in dynamic balance.
Postural stability depends on the integration of visual, deep sensory and vestibular signals, which leads to an appropriate motor response to counteract posture oscillation. (Shumway-Cook and Woollacot, 1995) Researchers argue that posture control is not fully automatic and needs some attention. (Pellecchia, 2003; Barra et al., 2006; Teasdale and Simoneau, 2001) The existence of attention in posture control is considered as one of the functions of high levels of perception because attention is needed for posture control to correct sensory input and produce appropriate motor output. (Huxhold et al., 2006) Performing a secondary cognitive task diverts attention away from balance symptoms, leading to disturbance in postural reactions and postural control. (Swan et al., 2004) It seems that doing and repeating exercises target conscious control mechanisms and attention strategies in postural control and reduce the role of automatic control in balance control. Thus, DTT causes plasticity in the motor cortex and primary cortical somatosensory and improves motor memory. (Elhinidi et al., 2016) In other words, in case of doing DTT, re-training the new ways happens and eventually improves the postural control more than doing the balance exercises alone. The present study obtained better results in postural control in DTT group.
In this study, there were no significant differences in the balance indices between the two groups after applying the changes, which can be attributed to the lack of evaluation of dynamic stability along with a cognitive task. In a study on people with ankle instability, Hung et al. (2016) showed that removing the visual feedback created by a Biodex monitor worsens balance control. Moreover, cognitive or physical disturbances can worsen stability indices in balance evaluation. (Hung and Miller, 2016) According to the study, because our exercises included cognitive training along with balance training, we might have seen more improvement in DTT group relative to the balance-training group if evaluation method had been done as dual-task.
Conclusion
DTT led to improvement in more balance indices studied compared to Biodex balance training. Thus, it is suggested to include DTT in the physiotherapy program for people with FAI. It is suggested to add a control group and evaluate during a cognitive task to better compare FAI role.
Table 1: Comparison of the demographic information between the two groups.
|
Variable |
Balance training group= 17 |
DTT group= 17 |
P value |
|
Mean ± SD |
Mean ± SD |
||
|
Age |
9.90 ± 31.06 |
34.82 ± 11.18 |
0.325 |
|
Height |
0.89 ± 1.64 |
0.89 ± 1.63 |
0.710 |
|
Weight |
19.39 ± 71.80 |
15.79 ± 70.38 |
0.821 |
|
BMI |
5.77 ± 26.37 |
5.52 ± 26.37 |
0.999 |
|
Gender f/m |
7/8 |
12/5 |
0.180 |
Table 2: Comparison of the data mean after and before the intervention for overall, anterior-posterior and lateral stability indices in the two groups and comparison of the results after the intervention between the two groups
|
Variable |
Balance training group |
DTT group |
Comparison of results after intervention |
||||
|
Before intervention |
After intervention |
P value ٭ |
Before intervention |
After intervention** |
P value ٭ |
P value ٭ |
|
|
OSIDO8 |
0.86 ± 1.50 |
0.58 ± 0.96 |
0.001 |
1.67 ± 0.86 |
0.92 ± 0.63 |
0.000 |
0.84 |
|
OSIDO5 |
1.70 ± 1.07 |
1.18 ± 0.92 |
0.000 |
1.90 ± 1.01 |
1.08 ± 0.88 |
0.000 |
0.76 |
|
OSIDC8 |
6.00 ± 4.47 |
4.96 ± 4.31 |
0.005 |
5.51 ± 3.72 |
3.60 ± 3.04 |
0.000 |
0.30 |
|
OSIDC5 |
9.83 ± 4.70 |
7.66 ± 5.17 |
0.001 |
9.04 ± 5.31 |
6.03 ± 4.74 |
0.000 |
0.36 |
|
OSISO8 |
2.14 ± 1.35 |
1.74 ± 0.96 |
0.006 |
1.87 ± 0.96 |
1.51 ± 0.83 |
0.005 |
0.49 |
|
OSISO5 |
2.70 ± 1.93 |
1.92 ± 1.20 |
0.005 |
2.33 ± 1.45 |
1.60 ± 1.02 |
0.000 |
0.42 |
|
APSIDO8 |
1.10 ± 0.72 |
0.42 ± 0.68 |
0.004 |
1.17 ± 0.61 |
0.62 ± 0.41 |
0.000 |
0.70 |
|
APSIDO5 |
1.26 ± 0.86 |
0.86 ± 0.67 |
0.001 |
1.28 ± 0.74 |
0.77 ± 0.55 |
0.000 |
0.68 |
|
APSIDC8 |
4.31 ± 3.46 |
3.27 ± 2.76 |
0.001 |
3.72 ± 2.15 |
2.49 ± 1.90 |
0.000 |
0.35 |
|
APSIDC5 |
6.73 ± 2.9 |
5.11 ± 3.6 |
0.001 |
5.96 ± 3.4 |
3.82 ± 2.7 |
0.000 |
0.26 |
|
APSISO8 |
1.32 ± 0.64 |
1.19 ± 0.75 |
0.008 |
1.31 ± 0.70 |
1.07 ± 0.57 |
0.026 |
0.60 |
|
APSISO5 |
2.41 ± 3.08 |
1.19 ± 0.72 |
0.231 |
1.60 ± 0.90 |
1.09 ± 0.74 |
0.000 |
0.70 |
|
MLSIDO8 |
0.81 ± 0.43 |
0.55 ± 0.33 |
0.002 |
0.92 ± 0.50 |
0.52 ± 0.42 |
0.000 |
0.86 |
|
MLSIDO5 |
0.88 ± 0.49 |
0.71 ± 0.53 |
0.148 |
1.07 ± 0.62 |
0.64 ± 0.53 |
0.000 |
0.70 |
|
MLSIDC8 |
3.34 ± 2.31 |
3.25 ± 2.69 |
0.789 |
3.21 ± 2.68 |
2.08 ± 2.06 |
0.003 |
0.17 |
|
MLSIDC5 |
5.70 ± 3.1 |
4.36 ± 3.4 |
0.012 |
5.41 ± 3.3 |
3.85 ± 3.1 |
0.001 |
0.66 |
|
MLSISO8 |
1.43 ± 1.18 ± |
1.02 ± 0.51 |
0.071 |
1.06 ± 0.63 |
0.84 ± 0.51 |
0.008 |
0.33 |
|
MLSISO5 |
1.82 ± 1.64 |
1.13 ± 0.71 |
0.087 |
1.35 ± 0.97 |
0.88 ± 0.59 |
0.001 |
0.29 |
* P<0.05 significant
** Mean and standard deviation
OSIDO8 = Overall Stability Index, Double leg stance with Opened eyes in level 8
OSIDO5 = Overall Stability Index, Double leg stance with Opened eyes in level 5
OSIDC8 = Overall Stability Index, Double leg stance with Closed eyes in level 8
OSIDC5 = Overall Stability Index, Double leg stance with Closed eyes in level 5
OSISO8 = Overall Stability Index, Single leg stance with Opened eyes in level 8
OSISO5 = Overall Stability Index, Single leg stance with Opened eyes in level 5
APSIDO8 = Anterior- Posterior Stability Index, Double leg stance with Opened eyes in level 8
APSIDO5 = Anterior- Posterior Stability Index, Double leg stance with Opened eyes in level 5
APSIDC8 = Anterior- Posterior Stability Index, Double leg stance with Closed eyes in level 8
APSIDC5 = Anterior- Posterior Stability Index, Double leg stance with Closed eyes in level 5
APSISO8 = Anterior- Posterior Stability Index, Single leg stance with Opened eyes in level 8
APSISO5 = Anterior- Posterior Stability Index, Single leg stance with Opened eyes in level 5
MLSIDO8 = Medio- Lateral Stability Index, Double leg stance with Opened eyes in level 8
MLSIDO5 = Medio- Lateral Stability Index, Double leg stance with Opened eyes in level 5
MLSIDC8 = Medio- Lateral Stability Index, Double leg stance with Closed eyes in level 8
MLSIDC5 = Medio- Lateral Stability Index, Double leg stance with Closed eyes in level 5
MLSISO8 = Medio- Lateral Stability Index, Single leg stance with Opened eyes in level 8
MLSISO5 = Medio- Lateral Stability Index, Single leg stance with Opened eyes in level 5
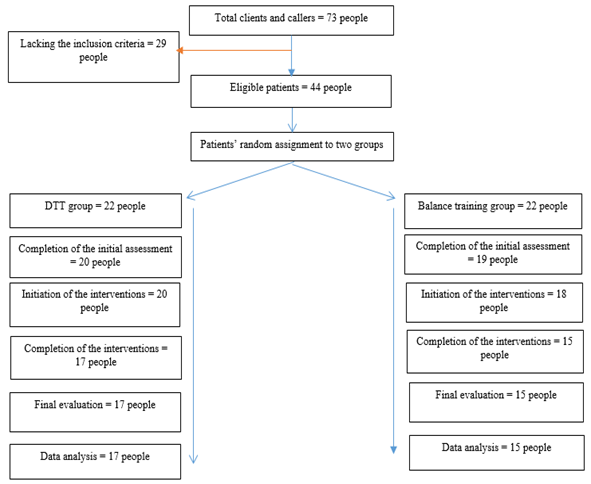
Figure 1: Process progression during this clinical trial
References
Akbari, A., Sarmadi, A., & Zafardanesh, P. (2014). The effect of ankle taping and balance exercises on postural stability indices in healthy women. Journal of physical therapy science, 26(5), 763-769.
Akhbari, B., Takamjani, I. E., Salavati, M., & Sanjari, M. A. (2007). A 4-week biodex stability exercise program improved ankle musculature onset, peak latency and balance measures in functionally unstable ankles. Physical Therapy in Sport, 8(3), 117-129.
Andersson, G., Hagman, J., Talianzadeh, R., Svedberg, A., & Larsen, H. C. (2002). Effect of cognitive load on postural control. Brain research bulletin, 58(1), 135-139.
Barra, J., Bray, A., Sahni, V., Golding, J. F., & Gresty, M. A. (2006). Increasing cognitive load with increasing balance challenge: recipe for catastrophe. Experimental Brain Research, 174(4), 734-745.
Beckman, S. M., & Buchanan, T. S. (1995). Ankle inversion injury and hypermobility: effect on hip and ankle muscle electromyography onset latency. Archives of physical medicine and rehabilitation, 76(12), 1138-1143.
Dault, M. C., Geurts, A. C., Mulder, T. W., & Duysens, J. (2001). Postural control and cognitive task performance in healthy participants while balancing on different support-surface configurations. Gait & posture, 14(3), 248-255.
Demeritt, K. M., Shultz, S. J., Docherty, C. L., Gansneder, B. M., & Perrin, D. H. (2002). Chronic ankle instability does not affect lower extremity functional performance. Journal of athletic training, 37(4), 507.
Docherty, C. L., McLeod, T. C. V., & Shultz, S. J. (2006). Postural control deficits in participants with functional ankle instability as measured by the balance error scoring system. Clinical Journal of Sport Medicine, 16(3), 203-208.
Eils, E., & Rosenbaum, D. (2001). A multi-station proprioceptive exercise program in patients with ankle instability. Medicine and science in sports and exercise, 33(12), 1991-1998.
Elhinidi, E. I. M., Ismaeel, M. M. I., & El-Saeed, T. M. (2016). Effect of dual-task training on postural stability in children with infantile hemiparesis. Journal of physical therapy science, 28(3), 875-880..
Farahpour, N., Ghazaleh, L., SABA, M. S., & Allard, P. (2004). The Effects of the Disturbance of the Vestibular System on the Dynamic Balance of Idiopathic Scoliotic Subjects with and Without Exercise Therapy Compared to Healthy Subjects.
Ferber, R., Osternig, L. R., Woollacott, M. H., Wasielewski, N. J., & Lee, J. H. (2003). Gait perturbation response in chronic anterior cruciate ligament deficiency and repair. Clinical Biomechanics, 18(2), 132-141.
Freeman, M. A. R., Dean, M. R. E., & Hanham, I. W. F. (1965). The etiology and prevention of functional instability of the foot. The Journal of bone and joint surgery. British volume, 47(4), 678-685.
Geurts, A. C., & Mulder, T. W. (1994). Attention demands in balance recovery following lower limb amputation. Journal of Motor Behavior, 26(2), 162-170.
Greve, J., Alonso, A., Bordini, A. C. P., & Camanho, G. L. (2007). Correlation between body mass index and postural balance. Clinics, 62(6), 717-720.
Gribble, P. A., & Robinson, R. H. (2009). Alterations in knee kinematics and dynamic stability associated with chronic ankle instability. Journal of athletic training, 44(4), 350-355.
Hagovská, M., & Olekszyová, Z. (2016). Relationships between balance control and cognitive functions, gait speed, and activities of daily living. Zeitschrift für Gerontologie und Geriatrie, 1-6.
Hale, S. A., Hertel, J., & Olmsted-Kramer, L. C. (2007). The effect of a 4-week comprehensive rehabilitation program on postural control and lower extremity function in individuals with chronic ankle instability. Journal of orthopaedic & sports physical therapy, 37(6), 303-311.
Heim, S., Pape-Neumann, J., van Ermingen-Marbach, M., Brinkhaus, M., & Grande, M. (2015). Shared vs. specific brain activation changes in dyslexia after training of phonology, attention, or reading. Brain Structure and Function, 1-17.
Hertel, J. (2002). Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. Journal of athletic training, 37(4), 364.
Huang, H. J., & Mercer, V. S. (2001). Dual-task methodology: applications in studies of cognitive and motor performance in adults and children. Pediatric Physical Therapy, 13(3), 133-140.
Hubbard, T. J., & Kaminski, T. W. (2002). Kinesthesia is not affected by functional ankle instability status. Journal of athletic training, 37(4), 481.
Hung, Y. J., & Miller, J. (2016). Extrinsic visual feedback and additional cognitive/physical demands affect single-limb balance control in individuals with ankle instability. World journal of orthopedics, 7(12), 801.
Huxhold, O., Li, S. C., Schmiedek, F., & Lindenberger, U. (2006). Dual-tasking postural control: aging and the effects of cognitive demand in conjunction with focus of attention. Brain research bulletin, 69(3), 294-305.
Huxhold, O., Li, S. C., Schmiedek, F., & Lindenberger, U. (2006). Dual-tasking postural control: aging and the effects of cognitive demand in conjunction with focus of attention. Brain research bulletin, 69(3), 294-305.
Ihara, H., Takayama, M., & Fukumoto, T. (2008). Postural control capability of ACL-deficient knee after sudden tilting. Gait & posture, 28(3), 478-482.
Jain, T. K., Wauneka, C. N., & Liu, W. (2016). Four weeks of balance training does not affect ankle joint stiffness in subjects with unilateral chronic ankle instability. International journal of sports and exercise medicine, 2(1).
Johansson, H., Sjölander, P., & Sojka, P. (1991). A sensory role for the cruciate ligaments. Clinical orthopaedics and related research, (268), 161-178.
Konak, H. E., Kibar, S., & Ergin, E. S. (2016). The effect of single-task and dual-task balance exercise programs on balance performance in adults with osteoporosis: a randomized controlled preliminary trial. Osteoporosis International, 27(11), 3271-3278.
Lajoie, Y., Teasdale, N., Bard, C., & Fleury, M. (1993). Attentional demands for static and dynamic equilibrium. Experimental brain research, 97(1), 139-144.
Lehman, G. J. (2006). Trunk and hip muscle recruitment patterns during the prone leg extension following a lateral ankle sprain: A prospective case study pre and post injury. Chiropractic & osteopathy, 14(1), 4.
Lysholm, M., Ledin, T., Ödkvist, L. M., & Good, L. (1998). Postural control—a comparison between patients with chronic anterior cruciate ligament insufficiency and healthy individuals. Scandinavian journal of medicine & science in sports, 8(6), 432-438.
Melzer, I., Benjuya, N., & Kaplanski, J. (2001). Age-related changes of postural control: effect of cognitive tasks. Gerontology, 47(4), 189-194.
O'Shea, S., Morris, M. E., & Iansek, R. (2002). Dual task interference during gait in people with Parkinson disease: effects of motor versus cognitive secondary tasks. Physical therapy, 82(9), 888-897.
Pellecchia, G. L. (2003). Postural sway increases with attentional demands of concurrent cognitive task. Gait & posture, 18(1), 29-34.
Rahnama, L., Salavati, M., Akhbari, B., & Mazaheri, M. (2010). Attentional demands and postural control in athletes with and without functional ankle instability. Journal of orthopaedic & sports physical therapy, 40(3), 180-187.
Rose, A., Lee, R. J., Williams, R. M., Thomson, L. C., & Forsyth, A. (2000). Functional instability in non-contact ankle ligament injuries. British journal of sports medicine, 34(5), 352-358.
Ross, S. E., Guskiewicz, K. M., & Yu, B. (2005). Single-leg jump-landing stabilization times in subjects with functionally unstable ankles. Journal of athletic training, 40(4), 298.
Rotem-Lehrer, N., & Laufer, Y. (2007). Effect of focus of attention on transfer of a postural control task following an ankle sprain. journal of orthopaedic & sports physical therapy, 37(9), 564-569.
Rowe, A., Wright, S., Nyland, J., Caborn, D. N., & Kling, R. (1999). Effects of a 2-hour cheerleading practice on dynamic postural stability, knee laxity, and hamstring extensibility. Journal of Orthopaedic & Sports Physical Therapy, 29(8), 455-462.
Rozzi, S. L., Lephart, S. M., Sterner, R., & Kuligowski, L. (1999). Balance training for persons with functionally unstable ankles. Journal of Orthopaedic & Sports Physical Therapy, 29(8), 478-486.
Schuhfried, G. (2007). CogniPlus. Schuhfried GmbH, Mödling.
Shehab, A. A. S. (2012). Attention Functions in Traumatic Brain Injury and Stroke: An Exploration of the Predictors of Daily Living Difficulties and the Correlates of the CogniPlus Vigilance Training Programme.
Shumway-Cook, A., & Woollacot, M. (1995). Motor Control: Theory and Practical Applications, Baltimore, MD: Williams and Wilkins.
Shumway-Cook, A., & Woollacott, M. (2000). Attentional demands and postural control: the effect of sensory context. Journals of Gerontology-Biological Sciences and Medical Sciences, 55(1), M10.
Sinaei, E., Kamali, F., Nematollahi, A., & Etminan, Z. (2016). Comparing the effects of balance training with and without cognitive tasks on the quality of life and balance performance in community-dwelling older adults: a single-blind randomized clinical trial. Journal of Rehabilitation Sciences & Research, 3(4), 91-96.
Sohlberg, M. M., & Mateer, C. A. (2017). Cognitive rehabilitation: An integrative neuropsychological approach. Guilford Publications.
Sturm, W., Fuhr, P., Zimmermann, R., & Gschwandtner, U. (2015). Cognitive training in Parkinson disease: Cognition-specific vs nonspecific computer trainingAuthor Response. Neurology, 84(1), 104-105.
Swan, L., Otani, H., Loubert, P. V., Sheffert, S. M., & Dunbar, G. L. (2004). Improving balance by performing a secondary cognitive task. British Journal of Psychology, 95(1), 31-40.
Teasdale, N., & Simoneau, M. (2001). Attentional demands for postural control: the effects of aging and sensory reintegration. Gait & posture, 14(3), 203-210.
Teasdale, N., Bard, C., LaRue, J., & Fleury, M. (1993). On the cognitive penetrability of posture control. Experimental aging research, 19(1), 1-13.
Vanicek, N., Strike, S., McNaughton, L., & Polman, R. (2009). Postural responses to dynamic perturbations in amputee fallers versus nonfallers: a comparative study with able-bodied subjects. Archives of physical medicine and rehabilitation, 90(6), 1018-1025.
Vaseghnia, A., Takamjani, E., & Sarrafzadeh, J. (2008). The Effect of Heel Height on Standing Balance Indices. Razi Journal of Medical Sciences, 15, 187-198.
Webster, K. A., & Gribble, P. A. (2013). A comparison of electromyography of gluteus medius and maximus in subjects with and without chronic ankle instability during two functional exercises. Physical therapy in sport, 14(1), 17-22.
Wikstrom, E. A., Tillman, M. D., & Borsa, P. A. (2005). Detection of dynamic stability deficits in subjects with functional ankle instability. Medicine and science in sports and exercise, 37(2), 169-175.
Willems, T., Witvrouw, E., Delbaere, K., De Cock, A., & De Clercq, D. (2005). Relationship between gait biomechanics and inversion sprains: a prospective study of risk factors. Gait & posture, 21(4), 379-387.
Woollacott, M., & Shumway-Cook, A. (2002). Attention and the control of posture and gait: a review of an emerging area of research. Gait & posture, 16(1), 1-14.
Youssef, N. M., Abdelmohsen, A. M., Ashour, A. A., Elhafez, N. M., & Elhafez, S. M. (2018). Effect of different balance training programs on postural control in chronic ankle instability: a randomized controlled trial. Acta of bioengineering and biomechanics, 20(2), 159-69.

